
Published: March 2025 | Last updated: May 2026
How soon do early HIV symptoms appear, and when can you test reliably?
Acute HIV symptoms appear 2 to 4 weeks after exposure and can include fever, sore throat, swollen lymph nodes, fatigue, and a flat pink-to-purple rash on the trunk. Many people have mild symptoms or none at all. Reliable testing windows vary by test type: rapid antibody home tests from about 6 weeks, lab antigen/antibody tests from about 4 weeks, per <a href="https://www.cdc.gov/hiv/testing/" target="_blank" rel="noopener noreferrer">CDC guidance</a>.
Acute HIV infection produces flu-like symptoms in many people roughly two to four weeks after exposure. A meaningful share of newly infected people feel nothing at all in this window, while others develop fever, sore throat, swollen lymph nodes, fatigue, and a flat or slightly raised pink-to-purple rash across the chest, back, or arms. That mix of common-looking symptoms and the gap before a test can reliably detect the virus is the part that confuses most readers searching for early signs. The article below walks through what acute HIV looks and feels like, what the rash actually looks like on light and dark skin, how acute infection differs from a seasonal cold or flu, what the typical window periods are for the main test types, and what to do when symptoms and timing point toward testing.
This article is published by stdrapidtestkits.com, which sells at-home STI testing kits. We recommend products based on fit-for-purpose for the reader's concern, not commercial benefit.
First, let's separate panic from biology
After a sexual encounter that felt risky, a broken condom, an unprotected hookup, or simply uncertainty about a partner's status, it is common to start scanning the body for signs. Anxiety can tighten the throat, raise the heart rate, and produce night sweats on its own. The mind is powerful, especially when shame or fear is mixed in.
Anxiety does not cause HIV symptoms. The virus follows a biological timeline.
Acute HIV infection (sometimes called primary HIV infection) typically begins two to four weeks after exposure. The virus enters the bloodstream, replicates rapidly, and the immune system begins producing antibodies. According to the U.S. Centers for Disease Control and Prevention, many people experience flu-like symptoms during this stage, while others feel nothing at all. Both patterns are well documented and equally common.
Sensations that surface within hours or a day of a feared exposure (a tight throat, a tense stomach, a sudden sweat at night) almost always trace back to anxiety. Acute HIV symptoms are not biologically possible until the virus has been replicating for roughly two weeks. If something feels off the next morning, stress is a far more likely explanation than infection.
What acute HIV actually feels like
When acute HIV does produce noticeable symptoms, they often feel like a heavy, deep-body version of flu rather than a head cold. People describe persistent low-grade fever, tender lymph nodes in the neck or armpits, and a fatigue that does not improve with rest. The symptoms tend to overlap (fever and sore throat together, fatigue with night sweats) and to last longer than a typical viral cold.
The most common acute symptoms reported in clinical studies and summarized by the HIV.gov symptoms overview include fever, chills, rash, night sweats, muscle aches, sore throat, fatigue, swollen lymph nodes, and mouth ulcers. Not everyone gets every symptom, and some people get only one or two.
| Symptom | How it commonly feels | Typical duration |
|---|---|---|
| Fever | Low to moderate, often 100 to 102 °F, sometimes with chills | Several days to two weeks |
| Sore throat | Persistent, often without congestion or cough | Several days |
| Swollen lymph nodes | Tender glands in neck, armpits, or groin | Days to several weeks |
| Fatigue | Heavy exhaustion not relieved by rest | One to two weeks |
| Rash | Flat or slightly raised pink, red, or purple patches on the trunk, face, or arms | One to two weeks |
| Night sweats | Drenching sweats that soak sheets | Intermittent during acute phase |
| Headache and muscle aches | Generalized, similar to flu but slower to resolve | One to two weeks |
| Mouth ulcers | Small painful sores on lips, tongue, or inside cheeks | Days to two weeks |
The HIV rash, up close
The rash is one of the more searched-for early symptoms, partly because it is visible and partly because it is hard to identify on sight. Clinicians describe the acute HIV rash as maculopapular: a combination of flat discolored patches (macules) and slightly raised bumps (papules). The pattern is usually symmetrical, appearing in similar distributions on both sides of the body, and it rarely blisters or crusts during the acute phase.
Color varies significantly with skin tone, which is part of why the rash gets missed. On lighter skin, the patches tend to appear pink to red. On medium and darker skin, they often look reddish-brown, dark purple, or deep brown, which can be subtler to spot without good lighting. The rash most commonly affects the torso, chest, back, and abdomen, along with the face, neck, and arms. It rarely appears on the palms of the hands or soles of the feet, and a palms-and-soles rash should actually raise suspicion for secondary syphilis rather than HIV (the two infections share transmission routes and are sometimes acquired together).
Mild itching can occur, but many people describe the acute HIV rash as barely itchy at all, which ironically makes it easier to overlook. The rash generally resolves on its own within one to two weeks. That disappearance does not mean the virus is gone; it means the initial immune response phase is ending. The virus continues to replicate, and a person in this window is highly transmissible. According to the NIH HIVinfo fact sheet on HIV and rash, a rash that appears during acute infection can also show up later as a side effect of antiretroviral medications, so the same visible symptom can mean very different things depending on when in the HIV journey it appears.
Three different rashes can show up over the course of HIV
Not every rash connected to HIV looks the same or carries the same urgency. Three distinct categories exist, and understanding which is which changes the right response.
The first is the acute HIV rash described above. It appears during primary infection, two to four weeks after exposure, as the immune system mounts its first response. It is rarely dangerous in itself. The challenge is that it disappears on its own and creates false reassurance, while the virus continues replicating in the background.
The second category involves rashes caused by opportunistic infections. Without effective treatment, HIV progressively damages the immune system, allowing pathogens the body would normally suppress to cause problems. Conditions like herpes zoster (shingles), molluscum contagiosum, persistent fungal skin infections, and (in advanced disease) Kaposi's sarcoma all produce skin changes in people living with HIV. Kaposi's sarcoma lesions typically appear as dark red, brown, or purple patches or nodules, and they signal that the immune system is already substantially compromised, not that infection is recent.
The third type is medication-induced. Modern antiretroviral therapy is highly effective, but some HIV medicines can cause skin reactions in the first few weeks of treatment. Most are mild pink or red patches that resolve on their own within a few weeks and do not require stopping the medication. In rare cases, however, a medication rash can signal a serious hypersensitivity reaction such as Stevens-Johnson Syndrome (SJS), which is potentially life-threatening. The callout below covers what to look for.
A rash that appears within days to weeks of starting a new HIV medication and is accompanied by fever, blistering skin, mouth or eye sores, or any difficulty breathing or swallowing requires emergency medical attention. These are warning signs of Stevens-Johnson Syndrome (SJS) or toxic epidermal necrolysis (TEN), rare but life-threatening hypersensitivity reactions. Go to an emergency room rather than stopping the medication on your own first; the emergency team will manage the medication change safely.
Flu or HIV? Why timing tells the real story
Every winter, urgent care clinics fill up with patients who have fever, fatigue, and sore throat. The vast majority have a seasonal viral illness. A small fraction have something else. Symptoms alone do not give you certainty. Timing does.
Acute HIV symptoms most often appear two to four weeks after exposure. Seasonal flu, by contrast, produces symptoms within one to four days of catching the virus. That difference is meaningful: a scratchy throat that begins three days after a sexual encounter is far more consistent with a common respiratory virus than with acute HIV. A flu-like illness that develops three weeks later, with tender neck glands and persistent low-grade fever, is more consistent with the acute HIV pattern.
| Feature | Seasonal flu | Acute HIV infection |
|---|---|---|
| Symptom onset after exposure | 1 to 4 days | 14 to 28 days, sometimes up to 6 weeks |
| Most common symptoms | Fever, cough, congestion, body aches | Fever, sore throat, swollen lymph nodes, fatigue, rash |
| Respiratory features | Often prominent (cough, congestion, runny nose) | Usually minimal or absent |
| Duration | 3 to 7 days, fully resolves | Several days to 2 weeks, then symptom-free phase begins |
| Long-term course | Resolves completely | Virus persists; without treatment, immune damage continues silently |
What else looks like an HIV rash
You cannot definitively identify an HIV rash just by looking at it. No one can, not from a photo, not from a description, not from a symptom checker. The acute rash looks almost identical to rashes caused by other viral infections, allergic reactions, heat exposure, medication side effects, and common skin conditions. What the rash looks like is one data point. When it appeared, and in what context, matters far more.
That said, there are patterns that raise or lower the likelihood of HIV involvement. The key contextual clues are timing and symptom clustering. An acute HIV rash rarely appears in isolation; it almost always comes alongside other features of acute retroviral syndrome. A rash on its own with no fever, no swollen lymph nodes, and no exposure history is far less likely to be HIV-related. The comparison table below summarizes the look-alikes worth knowing.
| Condition | Typical appearance | Timing and context | Key distinguishing feature |
|---|---|---|---|
| Acute HIV rash | Flat or raised pink, red, or purple patches; symmetric and diffuse | 2 to 4 weeks after possible exposure | Appears alongside flu-like cluster; resolves in 1 to 2 weeks |
| Heat rash (miliaria) | Densely packed tiny itchy bumps, often clear vesicles | During or after heat or humidity exposure | No fever or lymph node involvement; resolves with cooling |
| Drug reaction | Variable; often widespread red patches and bumps | Within days to weeks of starting a new medication | Direct timing link to a recently started drug |
| Secondary syphilis | Rough, reddish-brown spots | Weeks after a primary chancre sore | Classically affects palms and soles; not typically itchy |
| Pityriasis rosea | Larger oval herald patch then smaller patches in a Christmas-tree pattern | Spontaneous onset, no known exposure | Distinctive herald patch precedes the rest of the rash |
| Eczema | Dry, scaly, intensely itchy patches | Chronic or recurring | Personal or family history; appears in skin creases |
The window period: why testing too early misleads
Many readers search for an HIV test the moment they feel anxious, take it, and hope a negative result will bring relief. The hard truth is that testing too early can produce false reassurance. The test is not broken and the user has not done anything wrong. The issue is the window period.
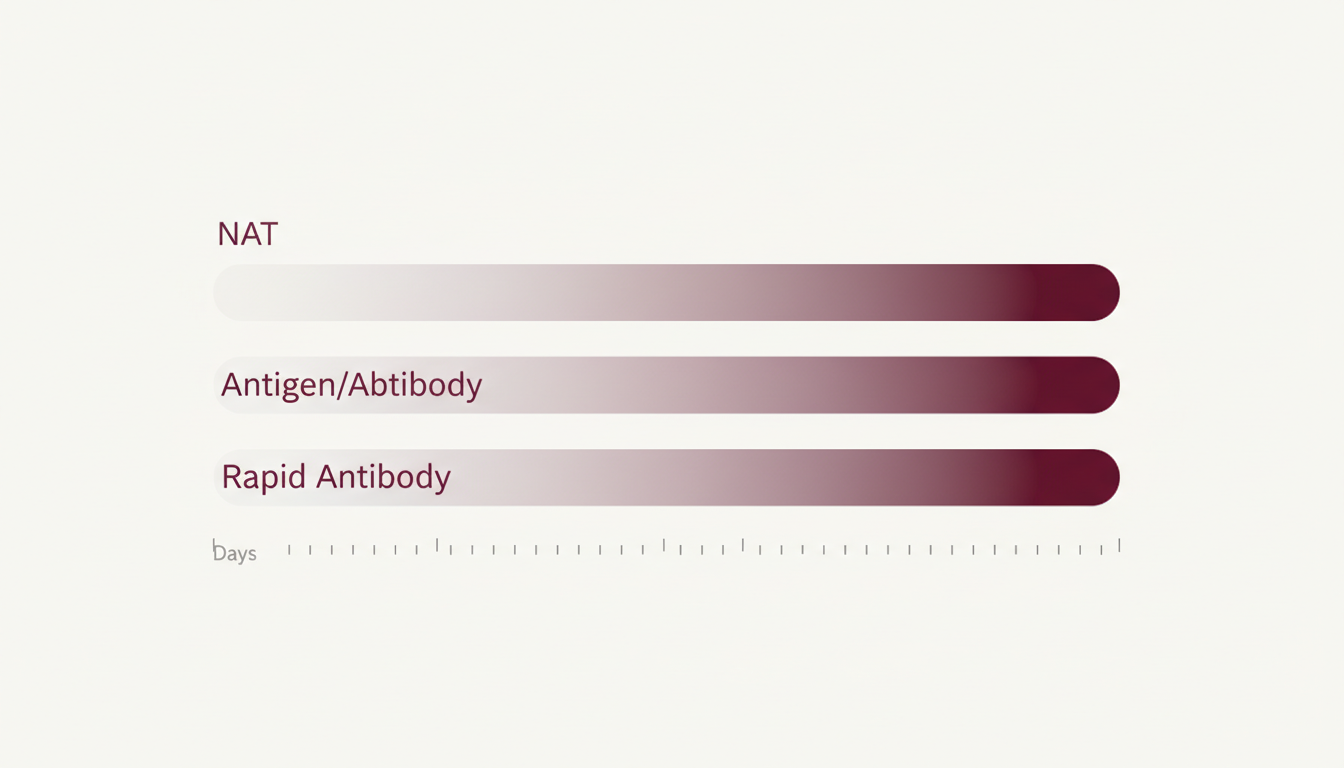
Every HIV test has a window period, the gap between exposure to HIV and when the test can reliably detect infection. During this gap, a person may already be infected, but the marker the test looks for (viral RNA, p24 antigen, or HIV antibodies) has not yet reached detectable levels. The CDC's testing overview publishes the typical window for each test type, and the ranges below reflect those values.
| Test type | What it detects | Typical window period | When results are most reliable |
|---|---|---|---|
| Nucleic acid test (NAT) | HIV RNA in blood | 10 to 33 days | Around 3 to 6 weeks after exposure |
| Lab antigen/antibody test | HIV p24 antigen plus antibodies | 18 to 45 days | Around 4 to 6 weeks after exposure |
| Antibody test (fingerstick or oral fluid, including FDA-approved at-home self-tests) | HIV antibodies | 23 to 90 days | Around 6 to 12 weeks after exposure |
What the window means after a recent exposure
The table above is the geometry, not the action plan. If a recent exposure is the reason you are reading this, the practical question is: given the test type you have access to and how long ago the exposure was, what does today's result actually mean? Two common mistakes are testing on day 3 and feeling falsely reassured by a negative, and waiting indefinitely because "what if the result is wrong." Both come from not matching the test type to the time elapsed.
If you are still within 72 hours of a higher-risk exposure, post-exposure prophylaxis (PEP) is the immediate priority, not testing. PEP is a 28-day course of HIV medicine that can prevent infection from taking hold when started within that 72-hour window. Contact a clinic, urgent care, or emergency room rather than waiting for symptoms to develop.
A negative rapid antibody test taken seven days after a possible exposure is essentially uninformative; the test cannot detect antibodies that have not yet formed. The same test taken at six weeks gives strong reassurance, and at twelve weeks the CDC considers a negative antibody result conclusive for most cases. If you tested early and the result was negative, schedule a follow-up at the appropriate window for your test type rather than treating the early result as final.

Managing the acute HIV rash while you wait to test
If the rash is part of the acute phase and you have not yet been able to test, the rash itself will likely resolve within one to two weeks without any specific intervention. Testing at the right window matters more than any home remedy, because a result lets treatment start if needed.
For symptom relief in the meantime, keeping the skin cool and well-moisturized helps reduce irritation. Avoiding direct sun exposure and very hot showers can prevent the rash from worsening. Over-the-counter hydrocortisone cream can reduce mild inflammation, and antihistamines may help if there is significant itching. These are comfort measures only; they ease the symptom without changing the underlying cause. If a clinician has already started you on antiretroviral therapy, never stop or alter any HIV medication without consulting your prescribing provider first, even if you suspect the medication is causing the rash. There are now multiple effective antiretroviral regimens available, and a rash from one option does not mean abandoning treatment altogether. Once viral load is suppressed below detectable levels, HIV cannot be transmitted sexually, the basis of the U=U principle (undetectable equals untransmittable) endorsed by both the CDC and WHO.
Keep skin cool and moisturized; avoid direct sun and hot showers to prevent worsening. OTC hydrocortisone can reduce mild inflammation, and antihistamines help if itching is significant. These manage symptoms only. Testing at the correct window (and any prescribed ART) addresses the underlying cause.
What HIV does not feel like
Clarity is calming, so the inverse list matters as much as the symptom list. Acute HIV does not typically cause thick genital discharge, sharp pelvic pain, an immediate burning sensation right after sex, or symptoms within hours of exposure. Those patterns point elsewhere.
If the main symptom is burning during urination within a day or two of unprotected sex, the more likely causes are bacterial infections such as gonorrhea, chlamydia, or a urinary tract infection. Clusters of painful blisters point more toward herpes. Intense itching with cottage-cheese-like discharge is usually yeast. Acute HIV is a systemic illness; it affects the whole body rather than producing one localized genital symptom. Fever, fatigue, and swollen lymph nodes are the more typical pattern.
An at-home or clinic test for chlamydia and gonorrhea is much higher-yield than an HIV test in this scenario. Both bacterial infections can produce burning within a few days of exposure, and both are easily treated once identified. A combined <a href="https://www.stdrapidtestkits.com/chlamydia-gonorrhea-home-test-kit">chlamydia and gonorrhea swab</a> can clarify the cause faster than continuing to monitor for HIV symptoms that almost certainly are not the source.
Symptoms in men and women: are they different?
Searches for "HIV symptoms in men vs. women" usually reflect a hope for clearer warning signs by gender. Acute HIV symptoms are largely the same in both, because the virus targets the immune system rather than reproductive organs. During acute infection, men and women alike may experience fever, fatigue, rash, sore throat, and swollen lymph nodes.
Differences appear later or in interpretation. Women with untreated HIV may develop recurring vaginal yeast infections, persistent bacterial vaginosis, or pelvic inflammatory disease that does not respond to standard antibiotics. Because these symptoms overlap with common gynecological complaints, HIV is sometimes not considered early in women, contributing to delayed diagnosis. Men with untreated HIV may notice persistent skin rashes, genital ulcers that do not heal, or earlier neurological changes such as memory difficulty.
For both genders, the absence of obvious genital symptoms does not rule out HIV, and routine screening matters whether or not the symptom pattern feels typical.
When anxiety amplifies symptoms
Anxiety produces real physical sensations. The throat tightens, the stomach churns, sweat pools at night, and every gland in the neck suddenly feels swollen on self-examination. After a feared exposure, this hyper-vigilance is almost universal. People press their lymph nodes repeatedly, scan their skin for rashes, and check their temperature five times a day.
Anxiety-driven sensations typically surface within hours or a day or two of the feared exposure, well before HIV is biologically possible, and they shift with mood rather than following the sustained week-long arc of a real acute illness. A fever persisting for a week and lymph nodes that stay tender for ten days are not anxiety; a throat that tightens while reading about HIV and eases when distracted almost certainly is.
Naming this pattern is not the same as dismissing it. The mind responds to fear with very physical signals, and recognizing that response is the first step toward stepping out of the loop and booking a properly timed test.
How HIV progresses if untreated
After the acute phase, untreated HIV typically enters a long clinical latency stage, sometimes called chronic HIV infection. Symptoms fade. The virus continues to replicate at lower levels and to slowly damage CD4 immune cells. People often feel completely well during this period, which can last several years to a decade or more depending on the individual and the strain. The NIH HIVinfo fact sheet on the stages of HIV infection describes this progression in detail, including the threshold for advanced disease.
Mild fatigue, persistent low-grade swollen lymph nodes, recurrent skin issues, and oral or genital ulcers can appear during this stage. None of these are specific to HIV, which is why routine screening (rather than symptom-spotting) is the standard public-health recommendation.
Without treatment, HIV eventually progresses to advanced disease (AIDS), defined by a CD4 count below 200 cells per cubic millimeter or by the appearance of an opportunistic infection. Symptoms at this stage include rapid weight loss, chronic diarrhea, recurring fevers, drenching night sweats, and infections such as tuberculosis or pneumocystis pneumonia.
Modern antiretroviral therapy (ART) interrupts that progression. People diagnosed early and started on consistent treatment can expect a long, healthy life, and once their viral load is suppressed below detectable levels, HIV cannot be transmitted sexually. This is the basis of the U=U principle (undetectable equals untransmittable), which the CDC and WHO both endorse.
Healthy adults have a CD4 T-cell count of roughly 500 to 1,500 cells per cubic millimeter of blood. As untreated HIV depletes these cells, opportunistic infections become progressively more common. Oral thrush and shingles often appear as the count drops below 500. Persistent fungal skin infections become common below 350. AIDS-defining conditions, including Kaposi's sarcoma, typically emerge below 200. A new, persistent, or atypical rash in someone known to be HIV-positive is a reason to check current CD4 status with their provider rather than wait it out at home.
Within 2 to 4 weeks after HIV infection, about two-thirds of people will have flu-like symptoms. This is the body's natural response to infection. Some people don't have any symptoms at all during this early stage of HIV.
So when should you actually test?
Match the test type to the time elapsed since exposure. For the earliest possible detection, a clinic-administered nucleic acid test (NAT) can identify HIV from about 10 days after exposure, with reliability climbing through three to six weeks. Lab antigen/antibody combination tests are reliable from about four to six weeks. Rapid antibody tests, including FDA-approved at-home self-tests, are most reliable from six weeks onward and considered conclusive at twelve weeks for most cases.
For routine screening without a specific exposure event, the CDC recommends that everyone aged 13 to 64 be tested for HIV at least once as part of standard healthcare, with annual or more frequent testing for people with ongoing risk factors (multiple partners, partners with HIV, men who have sex with men, injection drug use). The NHS HIV guidance and the WHO fact sheet describe similar screening logic for other regions.
If a recent exposure is the concern, the practical sequence looks like this: test at the earliest reliable window for the chosen test type (six weeks for an at-home rapid antibody kit), and if negative, retest at twelve weeks to confirm. Earlier tests can give preliminary information but should not be treated as final.

If the result is positive
A positive home test is a strong signal but not a final diagnosis. Every reactive at-home result needs confirmatory testing through a clinic or lab, typically with a lab antigen/antibody assay and a follow-up nucleic acid test. False positives on antibody-based tests are uncommon but do occur, which is why confirmation is the standard of care.
Modern HIV treatment has changed what this diagnosis means. With consistent antiretroviral therapy, people living with HIV can expect a long, healthy life. Most reach an undetectable viral load within months of starting treatment, which means they cannot transmit HIV to sexual partners. Linkage to care happens fast in most healthcare systems; primary-care clinics, sexual-health clinics, and infectious-disease specialists can all initiate treatment.
Emotionally, the first 24 hours after a reactive result feel heavy for almost everyone. What follows, though, is finite and well-mapped: confirmatory lab testing, a referral to an HIV care provider, and a treatment plan. (If the test was negative but the exposure was recent, the six- and twelve-week retest windows described above are the relevant follow-up points.) Acting quickly improves the long-term outcome.
1. Book confirmatory testing at a clinic or your primary-care provider, typically a lab antigen/antibody assay plus a follow-up nucleic acid test.
2. Ask the clinic to refer you to an HIV care provider; many systems can do this same-day, including primary-care, sexual-health, and infectious-disease clinics.
3. Discuss antiretroviral therapy at your first care appointment. Modern ART is highly effective and can suppress viral load to undetectable within months, which protects your health and prevents sexual transmission to partners.
Frequently asked questions about early HIV symptoms
- How soon after exposure do HIV symptoms appear?
- Acute HIV symptoms most often appear 2 to 4 weeks after exposure, occasionally up to 6 weeks. Many people have mild symptoms or none at all. Symptoms within the first three to five days after sex are far more likely to be from a common cold, flu, or anxiety than from HIV, because the virus has not yet had time to trigger an immune response.
- What does an HIV rash actually look like?
- A symmetrical scatter of flat and slightly raised spots, most often across the torso, chest, and back. On lighter skin the patches look pink to red; on medium or darker skin they appear reddish-brown to dark purple and can be easy to miss without good lighting. It rarely blisters, is often barely itchy, and clears within one to two weeks. That clearance does not mean the virus is gone. Only a properly timed test confirms the cause.
- How long does an HIV rash last?
- One to two weeks is the typical duration during the acute phase, sometimes less. When the rash clears, the acute immune-response phase is ending, but the virus is still present and replicating. Disappearance does not mean clearance. The right next step is to test at the 6-week post-exposure mark for a first meaningful result, then retest at 12 weeks if that result was negative.
- Can you get an HIV rash without any other symptoms?
- Yes, but it is uncommon. The acute phase almost always brings accompanying symptoms (fever, fatigue, swollen lymph nodes, sore throat) appearing together as acute retroviral syndrome. An isolated rash with no other symptoms and no known recent exposure is far more likely to have a non-HIV cause such as heat rash, a drug reaction, or pityriasis rosea. A test at the correct window is the only definitive answer.
- Can early HIV symptoms be mistaken for something else?
- Yes. The acute HIV symptom pattern (fever, sore throat, fatigue, swollen lymph nodes, rash) overlaps closely with flu, mononucleosis, strep throat, and even COVID-19. The features that point more toward HIV are the timing (two to four weeks after a possible exposure rather than one to four days) and the persistence of symptoms for one to two weeks rather than a few days.
- Does HIV cause burning during urination?
- Usually not. Burning during urination is far more typical of bacterial infections such as gonorrhea, chlamydia, or a urinary tract infection. Acute HIV is a systemic illness and tends to produce whole-body symptoms (fever, fatigue, swollen lymph nodes) rather than localized genital symptoms. If burning is the main complaint, the higher-yield tests are for chlamydia and gonorrhea.
- If I tested negative two weeks after exposure, can I trust the result?
- Only partially. At two weeks, a clinic-administered nucleic acid test (NAT) is approaching its reliable window, but lab antigen/antibody tests and rapid antibody home kits are still inside their window periods. A negative result at two weeks should be followed by a retest at the appropriate window for the chosen test type (6 weeks for at-home rapid antibody, 12 weeks for definitive confirmation).
- Do at-home HIV tests work?
- Yes, when used at the right time. FDA-approved at-home HIV tests use either a fingerstick blood sample or oral fluid to detect HIV antibodies and are designed for use from about six weeks after exposure, with most authorities considering a negative result at twelve weeks definitive. A reactive at-home result always requires confirmatory testing in a clinical setting.
- Can stress or anxiety mimic early HIV symptoms?
- Yes. Anxiety can produce very real fatigue, mild fever, sweating, throat tightness, and even hives. These sensations tend to appear within hours or days of a feared exposure (well before HIV symptoms are biologically possible), fluctuate with mood, and improve when the mind is distracted. If at least two to three weeks have passed since the possible exposure, book a test rather than continuing to monitor symptoms.
- What should I do if I think I have early HIV symptoms?
- Note when the possible exposure happened and when symptoms began. If you are within 72 hours of the exposure, contact a clinic about post-exposure prophylaxis (PEP) before anything else. Otherwise, if it has been at least two to three weeks since exposure, testing makes sense; choose a test type whose window matches the time elapsed (NAT at clinic for earliest detection, rapid antibody at home from six weeks, definitive at twelve weeks). If symptoms are severe (high fever, dehydration, neurological changes), seek in-person medical care; the workup will include HIV testing along with other infectious causes.
- U.S. Centers for Disease Control and Prevention. About HIV: stages of infection, acute symptoms, and treatment overview.
- U.S. Centers for Disease Control and Prevention. HIV testing overview, including window periods for nucleic acid, antigen/antibody, and rapid antibody tests, plus the 13 to 64 routine-screening recommendation.
- World Health Organization. HIV and AIDS fact sheet, including epidemiology, transmission, and global testing recommendations.
- HIV.gov. Symptoms of HIV: acute and later-stage symptom guidance, including the two-thirds-of-people figure quoted in the pull quote above.
- NHS (UK). HIV and AIDS: symptoms, testing, and treatment guidance for the United Kingdom.
- NIH HIVinfo. HIV and rash: description of the acute HIV rash as the body's immune response, and the role of medication-induced reactions during early ART.
