
Published: October 2025 | Last updated: May 2026
Which at-home STD test is best?
For a recent partner change with no symptoms, a multi-infection rapid panel covering the seven most common STIs is the most useful single screen. For symptomatic infection or pharyngeal/rectal exposure, see a clinic for NAAT instead. The right kit matches your exposure timing and the infections you need to rule out.
After a possible exposure, the question is rarely whether to test. It is which test, and when. Walk into a pharmacy or open a search tab and the choices stack up fast: rapid lateral-flow kits with results in 15 minutes, mail-in lab panels with NAAT chemistry, clinic visits with full provider workup. The right choice depends on which point in the timeline you are at, on which infection you are trying to rule out, and on whether an at-home STI test kit is the right fit for your situation in the first place.
This guide compares the three main routes by speed, privacy, accuracy, and clinical appropriateness. You will see when a 15-minute lateral-flow test is the right call, when a mail-in lab panel earns its longer wait, when a clinic visit is the only option that makes clinical sense, and where at-home kits stop being useful and start giving false reassurance.
Why people choose home testing over the clinic
Walking into a sexual health clinic is harder than it should be. For some, it is a question of distance: rural areas often have one clinic per county, and the next county over is a two-hour drive. For others, it is the receptionist line, the intake form that asks about partners, the fluorescent lighting, and the half hour spent in a waiting room with no clear answer to what comes next. Survey data on missed STI screening consistently puts inconvenience and stigma above cost as the leading reason, which is the same finding the CDC cites when explaining why its updated guidance now formally includes FDA-cleared self-test options.
At-home testing fills that gap. The kit arrives in plain packaging. You collect a sample at your kitchen counter, in a bathroom, or anywhere you have privacy. You read the result on a strip in 15 minutes, or mail the sample to a lab and check a portal a few days later. No receptionist, no waiting room, no shared elevator with a coworker who happens to be there.
Public-health bodies back the approach for the same reason. The CDC's STI testing guidance now covers FDA-approved self-test options and self-collection kits as ways to expand access for groups historically under-served by clinic-based programs (CDC STI testing). For readers who have experienced stigma in healthcare settings, including queer, trans, or non-monogamous patients, the privacy layer is often the entire reason home testing exists at all.
Self-care interventions, including self-collection of samples for sexually transmitted infections, expand access for people who may face barriers in clinic-based services.
How rapid kits, mail-in labs, and clinic tests compare
The three options use different chemistry and serve different moments. Rapid lateral-flow kits at home are immunoassays: a strip changes color when antibodies or antigens to a specific infection bind in the test region. Mail-in lab kits use the same molecular methods labs run for clinic samples (NAAT or PCR). Clinic visits add a clinician who can swab harder-to-reach sites, prescribe treatment on the spot, and interpret edge cases.
The trade-offs land in three places: how fast you get an answer, how many infections one kit covers, and what happens after a positive result.
| Test type | Sample | Time to result | Coverage | Best for |
|---|---|---|---|---|
| Rapid lateral-flow at home | Fingerstick blood or self-collected swab | 15 to 20 minutes | 1 to a small panel per kit | Single-infection screening, anxiety relief, off-grid privacy |
| Mail-in lab kit | Self-collected swab, urine, or fingerstick blood mailed to a CLIA-certified lab | 2 to 7 days | Multi-infection panels (often 6 to 10 STIs) | Comprehensive screening, partner-share documentation |
| Clinic visit with NAAT | Provider-collected or self-collected swab plus blood draw | 1 to 3 days | Tailored to symptoms and exposure history | Symptomatic infection, confirmatory diagnosis, immediate treatment access |
How rapid lateral-flow tests work
Two test technologies dominate the at-home category, and they work differently enough that it is worth understanding which one is in the box you ordered.
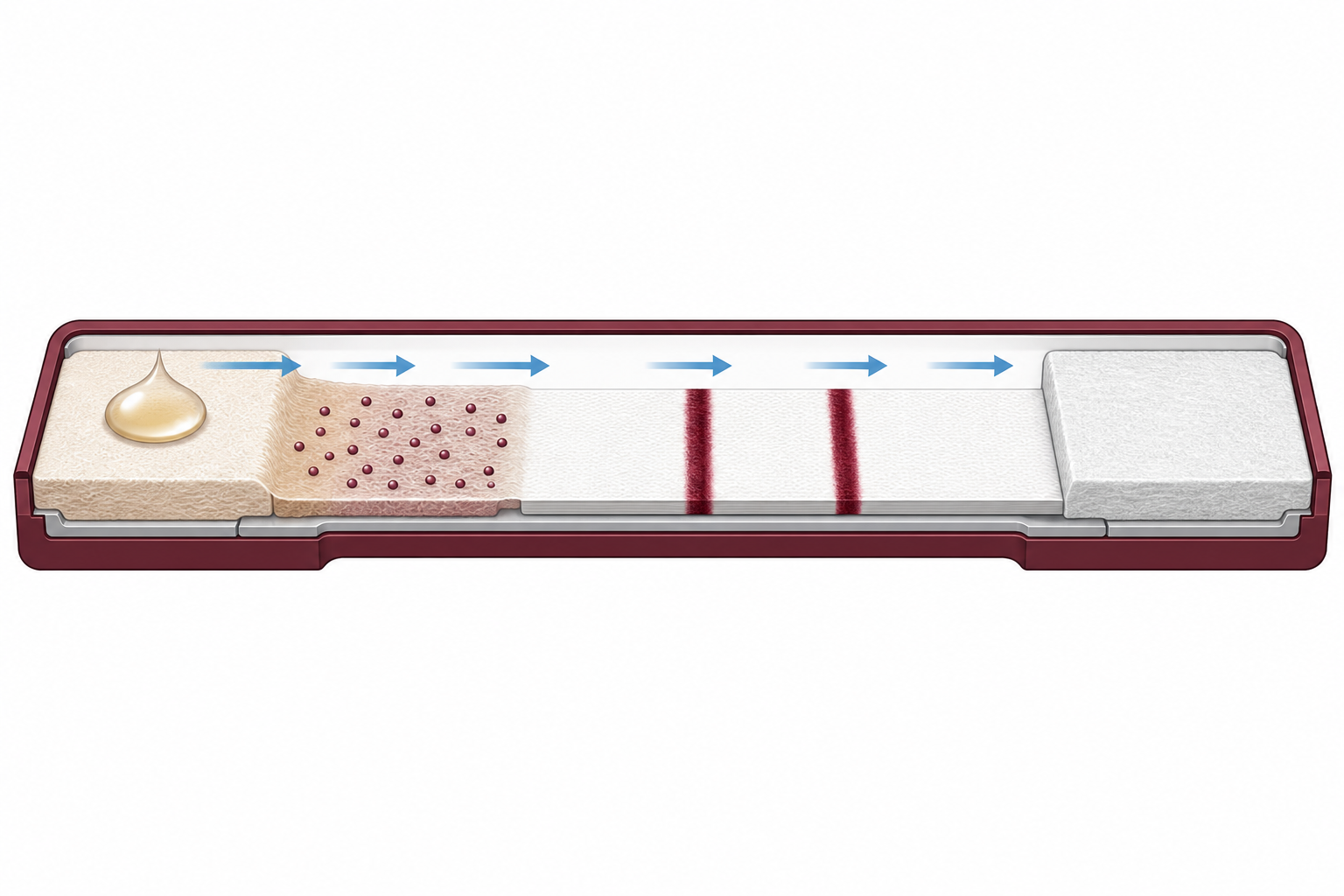
Rapid lateral-flow tests use the same chemistry as a home pregnancy test or a COVID antigen strip. A self-collected sample (a vaginal or penile swab for chlamydia and gonorrhea; a fingerstick blood drop for HIV, syphilis, hepatitis B, hepatitis C, and herpes) is mixed with a buffer and dripped onto a treated strip. Antibodies fixed on the strip bind to a target, either a pathogen antigen or your antibody response to the pathogen. If enough binding occurs above the kit's detection threshold, a colored line appears in the test window. A separate control line confirms the test ran correctly. The result reads in 10 to 20 minutes, no equipment needed.
Lab-processed tests (mail-in panels and clinic-collected samples) use NAAT, short for nucleic-acid amplification testing, or laboratory immunoassay. These methods amplify or detect very small amounts of pathogen DNA, RNA, or antibody, so they have higher analytical sensitivity than rapid lateral-flow strips, especially in the early window after exposure. The trade-off is processing time and a sample-handling chain you cannot see.
The two are complementary screening tools, not equivalent. A positive rapid test is a strong signal worth confirming with a lab NAAT before treatment. A negative rapid test outside the window period is reasonable evidence of clearance for screening purposes. Lab-based NAAT remains the reference standard for active infection diagnosis.
The infections you can screen for at home
At-home rapid kits cover the same seven infections that account for the majority of new diagnoses in the US each year. They split into two sample-type groups: swab-based (genital infections detectable from the mucosal surface) and blood-based (systemic infections detectable from a fingerstick antibody draw). Any kit that claims a single sample type for all seven is misrepresenting the chemistry.
Trichomoniasis and HPV are also available as at-home swabs, but validated for vaginal self-swab only; there is no FDA-cleared at-home male trichomoniasis or male HPV test on the market. Male readers concerned about either should see a clinician for a urethral, anal, or oropharyngeal swab. Mycoplasma genitalium, ureaplasma, bacterial vaginosis, and HPV strain typing are not in the at-home category and need a clinic visit.
HPV deserves its own framing. The CDC notes that long-lasting infection with certain types of HPV is the main cause of cervical cancer, and HPV infections are also linked to anal, oropharyngeal, and several other cancers (CDC cervical cancer overview). Routine cervical screening (Pap or HPV co-testing) and HPV vaccination address that cancer-prevention pathway separately from at-home STI screening, which is why HPV strain typing belongs in a clinic workflow rather than a rapid kit.
| Infection | At-home sample | What the test looks for | Typical window after exposure |
|---|---|---|---|
| Chlamydia | Self-collected swab | Bacterial antigen | 1 to 2 weeks |
| Gonorrhea | Self-collected swab | Bacterial antigen | 1 to 2 weeks |
| Syphilis | Fingerstick blood | Treponemal antibody | 3 to 6 weeks |
| HIV | Fingerstick blood | HIV antibody | 23 to 90 days for rapid antibody tests |
| Hepatitis B | Fingerstick blood | Surface antigen (HBsAg) | 4 to 12 weeks |
| Hepatitis C | Fingerstick blood | HCV antibody | 8 to 11 weeks |
| Herpes (HSV-2) | Fingerstick blood | Type-specific HSV-2 antibody | 6 to 12 weeks (up to 16 weeks for some assays) |
Window periods: when each infection becomes detectable
The window period is the time between exposure and when a test can reliably detect infection. Test inside the window and a negative result can mean either no infection or one that has not built up enough antibody, antigen, or genetic material to register. The window varies by pathogen and by test chemistry, which is why one calendar does not fit all (CDC HIV testing; the NHS STI overview covers the same point in plain English for non-US readers).
For chlamydia and gonorrhea, a NAAT can detect infection roughly one to two weeks after exposure. For syphilis, the antibody response takes longer; the standard recommendation is to test at three weeks at the earliest, with a definitive result by six weeks for most exposures and a final retest at twelve weeks for high-risk encounters. HIV testing depends on the assay generation: a NAAT can detect the virus by 10 to 33 days post-exposure; fourth-generation antigen/antibody tests detect by 18 to 45 days; rapid antibody-only tests can extend out to 90 days. HSV-2 antibody tests detect most seroconversions by 6 to 12 weeks per CDC guidance, with a small share of assays (notably some HerpeSelect-family kits) needing up to 16 weeks for a definitive rule-out.
The single biggest mistake people make with at-home testing is testing too early. If you cannot wait for the window to close because of a real clinical concern (not just anxiety), the right move is a clinic visit for early-window NAAT, not a rapid kit you will have to repeat anyway.
| Infection | Earliest reliable detection | Recommended test window | Retest needed? |
|---|---|---|---|
| Chlamydia | 1 to 2 weeks | 2 weeks after exposure | Only if first test was before 14 days |
| Gonorrhea | 1 to 2 weeks | 2 weeks after exposure | Only if first test was before 14 days |
| Syphilis | 3 weeks | 6 weeks (12 weeks for high-risk encounters) | At 12 weeks for definitive rule-out |
| HIV (NAAT) | 10 to 33 days | 2 to 4 weeks | At 90 days if test was very early |
| HIV (4th-gen antigen/antibody) | 18 to 45 days | 4 to 6 weeks | At 90 days for definitive rule-out |
| HSV-2 (antibody) | 6 weeks | 6 to 12 weeks (up to 16 for some assays) | At 16 weeks for definitive rule-out |
| Hepatitis B | 3 to 6 weeks | 6 weeks | Sometimes recommended |
| Hepatitis C (antibody) | 8 to 11 weeks | 12 weeks | Sometimes recommended |
Ready to screen once the window closes?
If you have hit the window and want to skip the clinic queue, the chlamydia and gonorrhea combo below is the most common starting point. The two bacterial infections co-occur often enough that screening for one without the other misses cases, and both windows close at roughly the same point (about 2 weeks post-exposure). This is the same at-home chlamydia and gonorrhea swab kit mentioned in the table above; sample is a self-collected swab, result reads in about 15 minutes, no lab portal involved.
STD Rapid Test Kits sells the at-home tests referenced in this article. We recommend products based on fit for the reader's concern, not commercial benefit, and call out where a clinic visit is the right choice instead.

Screening tool, not diagnostic tool
This is the section the marketing copy on most retailer sites skips. Knowing what an at-home kit does not do is as important as knowing what it does.
At-home rapid kits work well as a routine screen for the asymptomatic majority. They give people who would otherwise skip testing a discreet, low-friction way to know their status. They use the same swab or blood-drop sample type as the lab equivalents, processed at home in minutes instead of mailed for days. As a public-health tool, that shift is meaningful.
What they cannot do is replace a clinic visit when something is already wrong. Active symptoms (visible lesions, unusual discharge, painful urination, pelvic or testicular pain, fever) need diagnostic-precision lab testing and often same-day treatment. A rapid lateral-flow strip is not designed for that scenario. Neither is it designed to detect oral, throat, or rectal infection: no FDA-cleared at-home kit on the market includes a pharyngeal or rectal swab, so if your exposure was oral or anal sex and you are concerned about pharyngeal or rectal gonorrhea or chlamydia, the right test is a clinician-collected swab at a sexual-health clinic. We do not sell that kit and neither does any other at-home retailer we know of.
The category also does not match lab analytical sensitivity in the early window. Lab NAATs amplify pathogen DNA and can detect very small amounts; rapid lateral-flow strips need orders of magnitude more antigen or antibody to cross the detection threshold. A negative rapid test late in the window provides reasonable evidence of clearance for screening purposes. A negative rapid test early in the window does not. Used with realistic expectations as a screening tool for the asymptomatic majority, at-home kits add real value to the testing picture.
If you have visible lesions, unusual discharge, painful urination, pelvic or testicular pain, fever, or any other active symptom you suspect could be sexually transmitted, the right next step is a clinic visit, not a rapid kit. Active symptoms need diagnostic-precision lab testing and (where indicated) same-day treatment, neither of which an at-home screen provides.
How accurate are home STD tests, really?
Accuracy lives in two numbers: sensitivity (how often the test catches a real infection) and specificity (how often a negative really means uninfected). A test described as “99% accurate” without breaking those down is incomplete. The two numbers can move in opposite directions, and which one matters more depends on your reason for testing. The MedlinePlus STI overview makes a similar point: swab-based and blood-based tests are used for different infections, depending on what is being detected.
For self-collected samples, the headline finding from the literature is reassuring. Pooled analyses of self-collected vaginal swabs for chlamydia and gonorrhea find agreement with provider-collected swabs in the high 90 percent range when samples reach a CLIA-certified lab (a federally regulated clinical laboratory). The FDA has cleared at-home, self-collected STI testing devices for several common infections, and the CDC now lists FDA-approved self-test options as part of its STI testing guidance (CDC STI testing).
Lateral-flow rapid tests are a different category. They are immunoassays, not NAAT. For HIV and syphilis, lateral-flow chemistry is well-established and reads with high specificity after the appropriate window. For chlamydia and gonorrhea, lateral-flow rapid kits are useful as a screening step, and a positive result is typically followed up with a lab NAAT for confirmation before treatment. The same is true for trichomoniasis: a rapid result tells you something, and a NAAT confirmation tells you what comes next.
Three filters are worth applying before you click buy. First, FDA clearance or CE marking: either gives you confidence the manufacturer ran a controlled clinical validation study, not just internal QC. Second, the kit's assay-specific window in the instructions for use, which can shift by a week or two from the generic CDC ranges depending on assay generation. Third, sample-type accuracy: chlamydia and gonorrhea need a swab; the others need a fingerstick blood drop. Timing and follow-up are part of accuracy too. A test taken three days after exposure can be technically correct (no detectable antibodies yet) and still miss an early infection.
Lab NAAT and PCR sit at the top of the analytical-sensitivity ladder for bacterial STIs (chlamydia, gonorrhea, trichomoniasis). Lateral-flow rapid kits sit a step below for those same infections, and at the top for HIV and syphilis where the antibody and antigen targets are what the chemistry is designed for. Self-collected samples processed at a CLIA-certified lab perform comparably to provider-collected samples in published studies.
Reading your result without a clinician in the room
Lateral-flow rapid tests show two regions on a strip: a control line confirming the test ran correctly, and a test line that develops if the target antibody or antigen is present. A control line with no test line reads negative. A control line with a clear test line, even a faint one, reads positive. A control line that does not appear means the test failed and should be repeated with a fresh strip.
Faint test lines are the source of most second-guessing. The instinct is to tilt the strip toward the light, take a photo, post it on a forum, and hope someone calls it. The clinical reading is simpler: any visible test line within the read window listed in the kit instructions is a positive result. It does not matter how faint. Wait too long after the read window and a developing line can indicate evaporation rather than a real result, so set a timer and read the strip on time.
One detail buried in most kit instructions: the test you took has an expiration date and a temperature range. A kit that sat in a hot car or in a closet near a radiator can produce false readings even when used correctly. Check the expiration before opening the foil pouch, and if the kit has been stored outside its label range, replace it before testing.
A positive rapid HIV or syphilis test is preliminary by clinical convention. Confirmation with a lab NAAT or treponemal-specific assay is part of every diagnostic protocol. If a rapid result reads positive, do not start treatment, panic-text partners, or change your routine until a lab confirms. The follow-up usually takes a few days and changes nothing about the eventual outcome if positive, except that you will know with certainty.
Privacy: what each route does with your data
Privacy with home testing breaks into three layers: packaging, sample handling, and what happens to your record afterward. Most reputable kits arrive in plain envelopes with no STI branding and no labels visible to roommates or family members, so the packaging part of the question is the easy part. Most kits look like an ordinary online order on the doorstep.
Sample handling and recordkeeping are where the routes diverge. Mail-in lab panels create a digital record by design: the lab needs your name to match your sample, and your result lives in a portal you can log into. Some providers let you use a pseudonym; others require legal name for compliance. Lateral-flow rapid kits skip the data layer entirely. There is no sample to mail, no lab portal, no account. The result lives on a strip you can photograph, log, or discard.
If you are weighing privacy against follow-up support, the trade-off looks like this: lateral-flow rapid kits give you maximum control and minimum digital trail, with no built-in path to a telehealth visit if the result is positive. Mail-in lab kits add a clinician on the back end and a record in a portal. Clinics give you the most support and the largest record. There is no automatic public-health reporting from a self-administered rapid test. If you confirm a positive at a clinic, the clinician's report follows their jurisdiction's normal reporting rules.
What to do if your test is positive
A positive result is the start of a process, with a clear sequence of next steps. The first move depends on which infection and which test. For lateral-flow rapid tests on HIV and syphilis, a positive result is preliminary by clinical convention, and confirmation with a lab assay is the standard next step. For bacterial infections like chlamydia and gonorrhea, a positive home result generally goes through the same confirmation pathway: a NAAT at a clinic or via a mail-in kit, then antibiotic treatment if confirmed.
Most STIs are treatable. Chlamydia, gonorrhea, syphilis, and trichomoniasis clear with a single course of antibiotics. Hepatitis B and C have direct-acting antiviral regimens that work for most patients. HIV is a chronic but managed condition with single-tablet daily regimens that suppress the virus to undetectable levels. Herpes is lifelong but managed, with antivirals that suppress outbreaks and reduce transmission risk (WHO STI fact sheet). The earlier treatment starts, the lower the risk of complications and onward transmission.
The fertility-risk pathway is real but preventable. Untreated chlamydia or gonorrhea can ascend into the upper reproductive tract and trigger pelvic inflammatory disease (PID), a leading cause of tubal-factor infertility, ectopic pregnancy, and chronic pelvic pain. CDC treatment guidelines describe early antibiotic treatment as the most effective way to interrupt that progression, which is the underlying reason annual chlamydia and gonorrhea screening is recommended for sexually active women under 25 (CDC STD treatment guidelines).
The harder part is often telling a partner. The standard advice from clinicians is to lead with information and skip the apology. A partner notification looks like: “I tested positive for chlamydia. You should get tested too, and treated if positive. Here is what I know about timing.” Most people respond to that with gratitude rather than anger, and many local health departments offer notification services that deliver the message anonymously if you prefer. Per WHO STI guidance, partner treatment is a core part of breaking the transmission chain.
For HIV specifically, modern single-tablet daily antiretroviral therapy (ART) suppresses viral load to undetectable levels in the blood for most patients within three to six months of starting consistent treatment. The CDC states that if you have an undetectable viral load, you will not transmit HIV through sex, making sustained viral suppression the most effective way for people with HIV to stay healthy and protect partners (<a href="https://www.cdc.gov/hiv/treatment/index.html" target="_blank" rel="noopener noreferrer">CDC HIV treatment</a>).
When to retest, and how often
Retesting closes the loop in two situations: after an early test that may have fallen inside the window period, and after treatment to confirm clearance. The CDC recommends retesting for chlamydia and gonorrhea three months after treatment because reinfection from an untreated partner is common. For HIV, a definitive negative usually requires a follow-up at 90 days post-exposure if the initial test was earlier. For syphilis, RPR titer monitoring at three, six, and twelve months tracks treatment response.
For routine screening (no specific exposure event, just a wellness check), the CDC's screening guidance recommends annual testing for sexually active people, with more frequent testing for those with new or multiple partners, anyone living with HIV or on PrEP (pre-exposure prophylaxis, a daily medication that significantly reduces HIV risk), and anyone whose partner has tested positive. Every three to six months is a reasonable cadence for high-volume screening; once a year covers the baseline case (CDC STI testing).
Three common buying patterns cover most decisions. After a new partner with no specific concern, a multi-infection rapid panel works as a single screen once the relevant windows have closed (about 4 weeks covers most; 12 weeks covers all). After a known exposure to a specific infection, single-infection kits cost less and let you test the relevant window precisely; chlamydia plus gonorrhea is the most common pairing because the two often co-occur and have nearly identical windows. For routine annual screening with no specific concern, a chlamydia plus gonorrhea pairing is usually a better fit than a full panel. Keep a record of when you tested last, what you tested for, and what the result was. A note in your phone is enough.
Many STIs cause no symptoms. The only way to know whether you have one is to get tested.
Choosing the right panel for one-shot screening
If you would rather screen for everything in one go (after a long testing gap, before starting a new long-term relationship, or after a partner change with limited information), the 8-in-1 panel below adds HSV-1 and HSV-2 antibody testing on top of the seven-infection set. It is validated for both men and women, uses self-collected swabs plus a fingerstick blood sample, and is most useful once the relevant window periods have closed.

Quick decision aid: which route fits your situation
Three simple questions resolve most testing decisions. Walk through them in order; the first “yes” points you to the right route.
FAQs
- Can I trust the result of an at-home STD test?
- Reliability depends on timing as much as chemistry. Wait until the window period has closed, follow the kit instructions step by step, and a properly used at-home test gives a result you can act on. Positive rapid results still go to a lab NAAT before treatment starts, and any negative taken too early should be repeated once the appropriate window has passed.
- How accurate are at-home rapid STD tests compared to lab tests?
- At-home rapid lateral-flow kits sit a step below lab NAAT on the analytical-sensitivity ladder for bacterial STIs like chlamydia and gonorrhea, while lateral-flow chemistry for HIV and syphilis is well-established and reads with high specificity after the appropriate window. Performance varies meaningfully by infection and by kit, so check the assay-specific sensitivity and specificity on each product's instructions for use. A positive rapid result should be confirmed with a lab NAAT before treatment. The two technologies are complementary screening tools, not equivalent diagnostic tools.
- What is the fastest at-home STD test?
- Lateral-flow rapid kits return results in about 15 to 20 minutes from sample collection, with no shipping or lab portal involved. They are well-suited to single-infection screening and to situations where waiting days for an answer is not an option. The trade-off for speed is coverage: rapid kits typically test for one or a small panel of infections, while mail-in lab kits cover wider panels but take 2 to 7 days for results.
- How long after exposure should I wait before testing?
- Window periods vary by infection: 1 to 2 weeks for chlamydia and gonorrhea, 3 to 6 weeks for syphilis, 18 to 45 days for fourth-generation HIV antigen/antibody tests (up to 90 days for rapid antibody-only tests), 4 to 12 weeks for hepatitis B, 8 to 11 weeks for hepatitis C, and 6 to 12 weeks for HSV-2 antibody (some assays require up to 16 weeks). Testing inside the window risks a false-negative result. Always check the kit's instructions-for-use for the assay-specific window.
- Do at-home STD tests show up on insurance or medical records?
- Generally no, unless you choose to share the result with your insurer or doctor. Lateral-flow rapid kits create no digital record at all. Mail-in lab kits create a record in the provider's portal but do not bill insurance directly unless you submit a receipt for reimbursement. If avoiding any insurance footprint matters to you, paying out of pocket with a rapid kit or a self-pay mail-in lab is the cleanest path.
- Do at-home kits work for both men and women?
- Most do. Chlamydia, gonorrhea, syphilis, HIV, hepatitis B, hepatitis C, and herpes single-infection kits are validated for both. Trichomoniasis and HPV at-home kits are validated for vaginal self-swab only and do not have a male-compatible version on the market. Male readers concerned about either should see a clinician for a urethral or anal swab.
- What should I do if my at-home test is positive?
- See a clinician for confirmatory lab testing and to start treatment if confirmed. Most STIs detected on screening are treatable, and starting treatment promptly reduces the risk of complications and onward transmission. The clinician can also help with partner notification, which is a core part of breaking the transmission chain. Do not start antibiotics, panic-message partners, or change your routine until a lab confirms.
- Can I use an at-home test instead of seeing a clinician?
- For routine asymptomatic screening, yes. For active symptoms (lesions, discharge, pain on urination, fever) or oral, throat, or rectal exposure concerns, no. Symptomatic infection needs diagnostic-precision lab testing and often same-day treatment, neither of which a rapid lateral-flow test provides. Pharyngeal and rectal infections require clinician-collected swabs, which no at-home kit on the market includes.
- How often should I retest?
- The CDC recommends annual chlamydia and gonorrhea screening for sexually active women under 25 and for higher-risk adults of any age. People with multiple partners or known high-risk exposures should screen every 3 to 6 months. HIV testing is recommended at least once for everyone aged 13 to 64, and more often for higher-risk groups. After treatment for chlamydia or gonorrhea, retest at three months because reinfection from an untreated partner is common.
- U.S. Centers for Disease Control and Prevention. STI testing guidance covering FDA-approved self-test options, self-collection kits, and home-testing access for HIV, syphilis, chlamydia, gonorrhea, and trichomoniasis, plus screening intervals for asymptomatic adults.
- U.S. Centers for Disease Control and Prevention. HIV testing guidance covering window periods for NAAT, fourth-generation antigen/antibody, and rapid antibody-only tests.
- U.S. Centers for Disease Control and Prevention. HIV treatment overview, including the role of antiretroviral therapy in achieving an undetectable viral load and preventing sexual transmission.
- U.S. Centers for Disease Control and Prevention. Cervical cancer overview describing long-lasting HPV infection as the main cause of cervical cancer, and HPV's link to anal, oropharyngeal, and other cancers.
- U.S. Centers for Disease Control and Prevention. STD treatment guidelines, including diagnostic and therapeutic recommendations for chlamydia, gonorrhea, syphilis, herpes, and viral hepatitis.
- World Health Organization. Sexually transmitted infections fact sheet covering global prevalence, transmission, and partner-treatment guidance.
- National Health Service (UK). Plain-language consumer guide to STI testing, including symptoms, window periods, and when to seek testing.
- National Library of Medicine (MedlinePlus). Sexually transmitted infections overview covering symptoms, transmission, and the swab- and blood-based tests used in clinical diagnosis.
