
Published: May 2020 | Last updated: April 2026
Can you catch an STI from bed sheets?
For practical purposes, no. Sexually transmitted infections require direct contact with mucous membranes, broken skin, or specific body fluids. The pathogens behind chlamydia, gonorrhea, syphilis, HIV, herpes, HPV, and hepatitis B and C either inactivate too quickly on dry fabric or have no documented route from bedding to a new host. The CDC states explicitly that you will not get herpes from toilet seats, bedding, or shared towels. If you are worried about a real exposure (a recent unprotected encounter, a partner's diagnosis, an active symptom), test for the right infection at the right window. The bedding angle is almost always a distraction from what actually happened.
You check into a hotel, sit on the bed, and the thought hits you. Someone slept here last night. Could a bedsheet, a pillowcase, a damp towel, hand you a sexually transmitted infection? It is one of the most-asked questions on health forums and one of the quietest 2am worries. The honest answer reads boring, which is itself reassuring. Sexually transmitted infections almost universally need direct contact with mucous membranes, broken skin, or specific body fluids. Bed sheets do not provide that route in any meaningful way for the infections people fear.
This article walks through the science, the small-print exceptions (pubic lice and scabies), and what to do if your worry is really about a recent contact rather than the linens.
Why "STDs from bed sheets" is the question
The phrase clinicians use for what readers are really asking about is fomite transmission. A fomite is any inanimate object (a sheet, a towel, a doorknob, a toilet seat) that could in theory carry an infection from one person to another. Some pathogens do transmit this way: rhinoviruses (the cold), influenza, norovirus, and certain skin organisms like staph and MRSA. Sexually transmitted infections largely do not.
The CDC's overview of sexually transmitted infections lists transmission as occurring through vaginal, oral, and anal sex, plus intimate physical contact (CDC, About STIs). It does not list bedding. The WHO's STI fact sheet enumerates the same broad categories: sexual contact, mother-to-child during pregnancy or delivery, and unsafe blood transfusion (WHO, STI fact sheet). The NHS overview reads the same way (NHS, STIs). Three major public-health bodies, three lists of transmission routes, none mention sheets.
The CDC's herpes page goes a step further and addresses the question directly: "You will not get herpes from toilet seats, bedding, or swimming pools. You also will not get it from touching objects, such as silverware, soap, or towels" (CDC, About Genital Herpes). That language is unusually direct for an agency. It exists because the question is asked so often, and because the alternative explanation (a partner who did not disclose, an exposure the reader does not want to acknowledge) is harder to sit with than blaming the linens.
The CDC, WHO, and NHS describe the same broad transmission categories for sexually transmitted infections: sexual contact, mother-to-child transmission during pregnancy or delivery, and unsafe blood exposure. Bedding does not appear on any of the three lists.
The four routes STIs use
For nearly every infection people worry about, transmission requires one of four direct routes:
- Sexual contact with the genitals, mouth, or anus of an infected person, including during asymptomatic shedding for viral infections like HSV.
- Direct skin-to-skin contact with an active lesion or affected area (HPV warts, herpes sores, primary syphilis chancres).
- Blood-to-blood contact: shared injection equipment, occupational needlestick, transfusions in settings that do not screen blood, contaminated tattoo or piercing equipment.
- Mother-to-child transmission during pregnancy, delivery, or breastfeeding.
Bed sheets do not appear on any major agency's list because transmission via fabric has not been documented in any meaningful epidemiological dataset. Survival of a pathogen on a surface is not the same as ability to infect; the pathogen still has to reach a mucous membrane in viable concentration to cause an infection.
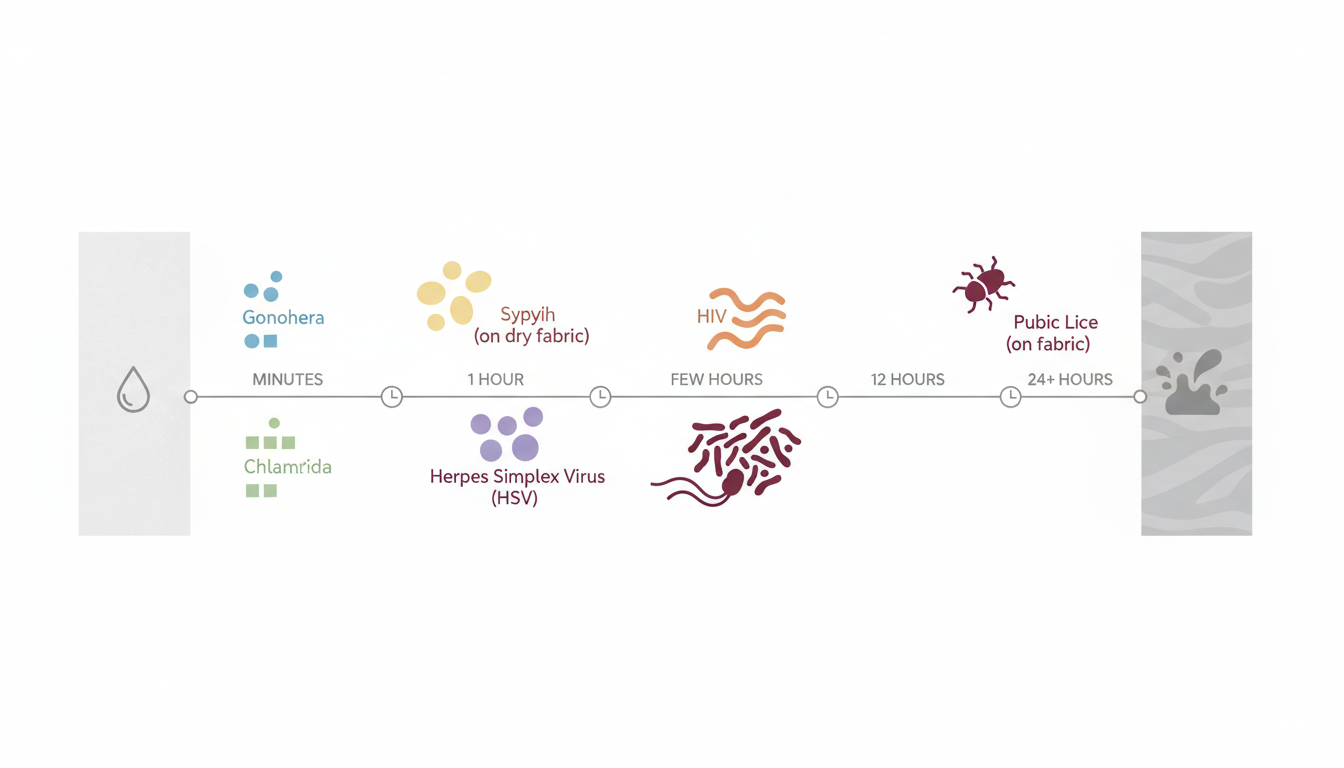
How long STI pathogens survive on fabric
Survival numbers from laboratory studies describe ideal conditions: warm, humid, freshly deposited fluid, short transit. Real-world bed sheets are dry, often air-exposed, often laundered between users in commercial settings. Even when a pathogen technically survives on a swatch of fabric in a controlled experiment, no real-world transmission case is recorded for any of the major STIs from clean bedding. The table below summarizes the rough survival picture and whether bedding transmission has been documented.
| Pathogen | Approximate survival outside body | Documented bedding transmission? |
|---|---|---|
| HIV | Inactivates within minutes to hours on dry surfaces | No |
| Gonorrhea (N. gonorrhoeae) | Hours under warm, moist lab conditions | No |
| Chlamydia trachomatis | Hours under warm, moist conditions | No |
| Syphilis (T. pallidum) | Minutes once dry; very fragile | No |
| Herpes simplex (HSV-1, HSV-2) | Brief on dry surfaces; longer if moist | No |
| Hepatitis B virus | Days on surfaces with dried blood (blood-borne route) | Not from clean linens |
| Hepatitis C virus | Up to several weeks in dried blood (lab data) | Not from clean linens |
| Trichomonas vaginalis | Up to about 24 hours on damp fabric (lab) | No documented cases |
| Pubic lice (Pthirus pubis) | Up to 24 to 48 hours off a host | Possible but uncommon |
Hotel sheets, hostel beds, and Airbnbs
The setting changes the anxiety, not the biology. Commercial hotel chains typically launder linens at roughly 160°F (71°C) or higher with detergents and oxidizing bleaches. Those conditions inactivate the bacteria, viruses, and protozoa we have been discussing. Even budget properties cycle linens through industrial laundry on a per-stay basis as a regulatory and reputational baseline.
Hostels, capsule rooms, and short-term rentals are more variable. The honest answer is the same: the actual measured risk for STI transmission from any bedding is so low that the public-health literature does not produce case reports of it. What you can plausibly pick up from a poorly-cleaned room is bedbugs, scabies, ringworm, or environmental staph (think MRSA on a bath mat). Those are skin and pest issues, not STIs, and they have very different prevention and treatment paths.
If a recent stay is on your mind because something feels physically wrong since you got home, ask instead what other contact happened on the trip, not what the housekeeper missed. The fear of the linens is often a stand-in for a harder conversation with yourself or a partner, and a home test answers that conversation more usefully than another inspection of the bedding.
We sell rapid at-home STI test kits; the products referenced below are from our own catalog.
Industrial laundering at 160°F (71°C) inactivates the bacteria, viruses, and protozoa that cause the STIs people fear. It does not, on its own, address bedbugs, scabies mites in mattress seams, or environmental staph on bath mats and tile. Those are the realistic shared-room concerns, and they have nothing to do with sexual contact.

The two real exceptions: pubic lice and scabies
Pubic lice and scabies are the small print of this conversation. Both are sometimes grouped with STIs because sex is their most common transmission route, but unlike chlamydia or gonorrhea they are insects and mites that can survive briefly off a human host.
The CDC notes pubic lice die within 24 to 48 hours without a blood meal, but during that window they can theoretically spread through "clothing, bedding, or (very rarely) using a toilet seat" recently used by an infested person (CDC, About Pubic Lice). Scabies mites can survive up to two to three days off human skin under typical conditions (CDC, About Scabies). Documented non-sexual transmission of either is uncommon and almost always involves close, prolonged contact such as shared sleeping arrangements among family members, not a single hotel stay or a brief use of a public towel.
If you find tiny crawling specks on bedding, intense itching especially at night, or pinpoint red marks in clusters, that is a clinical evaluation question. It is not one our home test kits answer; both lice and scabies are diagnosed visually or with a skin scrape, not a swab or blood draw. A primary-care visit or a dermatology referral is the right next step.
Note on the trichomoniasis exception: trichomoniasis has the longest documented off-host survival among the bacterial and protozoal STIs, up to about 24 hours on damp fabric in controlled laboratory conditions, yet there are still no documented real-world bedding transmission cases. Per the CDC, transmission requires a vaginal-to-vaginal, vaginal-to-penile, or penile-to-vaginal route in real life.
Pubic lice and scabies are the only STI-adjacent conditions with any documented (if uncommon) fomite spread. Both are diagnosed by direct visual inspection or a skin scrape rather than a swab or blood test. If you suspect either, book a primary-care or dermatology appointment.

When the symptom IS something (but probably not from the sheets)
Most people do not search "STD from bed sheets" out of pure curiosity. They search it because something feels off, and naming the linens is gentler than naming a partner. Here is the honest read on what is more likely behind common post-trip or post-sleepover symptoms.
- Genital itch or rash without pain. Often a contact reaction to an unfamiliar laundry detergent, fabric softener, scented body wash, condom material, or a new lubricant. Yeast overgrowth is also common after travel, antibiotic courses, or hot weather.
- Sudden burning during urination. A urinary tract infection is more likely than gonorrhea or chlamydia in someone with no recent sexual exposure. Both deserve testing if any sexual contact is in scope.
- Small clustered blisters or sores. Worth a clinical look. HSV is one possibility, but folliculitis, ingrown hairs from waxing, contact dermatitis, and shingles are also candidates depending on the location.
- Unusual discharge. Bacterial vaginosis, yeast, and trichomoniasis are far more common than gonorrhea or chlamydia among average sexually active people, and the differential really matters for treatment.
- Pinpoint marks in lines or clusters. Likely bedbug bites, especially if itchy and on body parts not covered by clothing. Report this to the property manager and move on; it is a hospitality and pest-control issue, with no swab or blood test needed.
- Generalized fatigue, sore throat, or fever within a couple of weeks of a real sexual exposure. Acute HIV seroconversion or a primary syphilis presentation is worth ruling out. This is the symptom pattern that should prompt testing, not the rash on day 3 of a beach holiday.
If a symptom started before any new sexual contact happened, the cause is almost certainly not an STI. Get it looked at by a clinician for accurate diagnosis rather than spiraling on a forum.
When testing actually makes sense (and which test fits)
If you have had a real exposure in the last few months (a new partner, a partner who tested positive, unprotected contact, a known incident), testing is the right call. It is not the right call because of bed sheets.
The window-period basics for the most common screens:
- Chlamydia and gonorrhea: detectable from about 14 days post-exposure on a swab.
- Trichomoniasis: detectable from about 7 to 14 days post-exposure.
- Syphilis: blood antibodies appear at 3 to 6 weeks; test at 6 weeks for confidence and retest at 3 months if negative and the exposure was high-risk.
- HIV: fourth-generation laboratory tests detect by 18 to 45 days; antibody-only home tests typically need 23 to 90 days; retest at 3 months for full confidence.
- HSV-2: blood antibody seroconversion takes 12 to 16 weeks on most assays for reliable results; a minority of people seroconvert by 6 to 8 weeks, so an earlier negative should be repeated at 12 weeks.
- Hepatitis B and C: antibody appearance is usually 8 to 12 weeks, with a 6-month retest after high-risk exposures.
Our at-home rapid kits are lateral-flow immunoassays. They are useful for screening on a plausible exposure timeline, with one important framing: any positive on a rapid home test is worth confirming with a laboratory NAAT or a clinician's repeat blood draw. A negative on the wrong side of the window period should be repeated when you cross the window. Lab NAAT remains the analytical gold standard for chlamydia and gonorrhea; the at-home rapid is the screening complement, not an equivalent.

Practical hygiene without going overboard
The realistic, non-paranoid rules for shared lodging and shared spaces:
- Wear pajamas or underwear in unfamiliar beds. The aim is to reduce skin-to-fabric contact and give yourself one less thing to worry about, with no claim that a layer of cotton blocks pathogens on its own.
- Use your own face cloth for eye and nasal areas. Conjunctival infections (gonococcal or chlamydial conjunctivitis) are rare in adults but not zero, and your own face towel is simply easier than cataloging hotel laundry standards.
- Do not sit naked on a damp towel that has been balled up on a tile floor. This is more about fungal and bacterial skin issues (athlete's foot, staph) than STIs.
- Wash your own bedding in hot water once a week. Wash a partner's clothing or shared linens on the warmest cycle the fabric tolerates after any active genital infection or skin condition.
- Do not share razors, period underwear, or anything that can break skin. This matters far more for blood-borne risk (hepatitis B, hepatitis C, HIV) than for surface-deposit risk.
- Clean shared sex toys between partners and between body sites. This is the closest thing to a real fomite-style STI exposure most people will encounter, and it is fully under your own control. Soap and water plus drying time is the baseline; toy-specific disinfectants exist for porous materials.
That is the entire list. There is no need to bring a hazmat kit on vacation.
Of all the hygiene steps above, the one with the largest measurable impact on STI risk has nothing to do with bedding: consistent condom use during new partnerships, frank conversations with partners about recent test results, and screening on a regular cadence rather than waiting for a symptom or a scare.
Myths worth retiring
- "You can catch HIV from a couch or sheet someone bled on." HIV is fragile outside a host. The CDC notes the virus does not survive long on environmental surfaces and cannot reproduce outside the human body. Documented surface-related HIV transmission involves shared injection equipment, not stained furniture.
- "Hotel cleaning is too rushed to kill STIs on linens." Most STIs are not transmitted by linens at any cleaning standard, including unclean. Industrial laundering at 160°F destroys the relevant pathogens regardless of the standard.
- "A toilet seat can give you chlamydia." Chlamydia trachomatis dies quickly outside the body and requires direct mucosal contact. There is no documented case of toilet-seat transmission, despite generations of anxiety about it.
- "If a sheet looks clean, it is clean." The look of a sheet says nothing about whether it has been laundered between guests. The relevant signal is the venue's laundry policy, not the visual whiteness of the linen.
- "A rash after a hotel stay is probably an STI." It is far more often a detergent reaction, a yeast or fungal flare, an insect bite, or contact with an unfamiliar body wash. STI is the least likely cause of a brand-new rash with no other risk factors.
You will not get herpes from toilet seats, bedding, or swimming pools. You also will not get it from touching objects, such as silverware, soap, or towels.
FAQs
- Can you catch an STI from a bed sheet?
- For practical purposes, no. The CDC and WHO list direct sexual contact, mother-to-child transmission, and unsafe blood transfusion as the routes that matter; bedding is not on either list. The CDC's herpes page is explicit that you will not get herpes from bedding or shared towels, and the same biology applies to chlamydia, gonorrhea, syphilis, HIV, HPV, and hepatitis B and C in real-world conditions.
- What about hotel or hostel sheets specifically?
- The biology is identical. Industrial laundering at roughly 160°F (71°C) inactivates the relevant pathogens, and even unwashed bedding does not provide the route an STI needs to reach a new mucous membrane. What you can plausibly catch from a poorly-cleaned room is bedbugs, scabies, athlete's foot, or environmental staph. Those are skin and pest concerns with their own evaluation paths, not STIs.
- Which STIs survive longest on fabric?
- Trichomonas vaginalis can survive on damp fabric for up to about 24 hours under laboratory conditions, the longest of the bacterial and protozoal STIs. Pubic lice can live up to 24 to 48 hours off a host. Hepatitis B and C can remain viable in dried blood for days to weeks, but they require a blood-to-blood entry route to infect, not surface contact.
- Can you get HIV from a bloodstain on a couch or sheet?
- No. The CDC notes HIV does not survive long on environmental surfaces and cannot reproduce outside a human host. Even fresh blood quickly loses the conditions HIV needs to remain infectious in air. Documented HIV transmission outside healthcare or sexual contact involves shared injection equipment, not stained furniture or laundry.
- Should I bring my own pillowcase when I travel?
- Not for STI prevention. There is no clinical reason to. If a personal pillowcase helps you sleep better in a strange room, it is its own reward; just do not let the routine convince you that hotel bedding is a real STI risk. It is not.
- I woke up with a rash after a stay. Should I assume it is an STI?
- Treat that as the least likely explanation. Detergent or fabric-softener reactions, yeast or fungal flares from heat and humidity, bedbug bites, contact dermatitis from a new soap, and folliculitis are all far more common. If a rash is in the genital area and persists, a clinician's look is the right next step. If you also had a recent sexual exposure on the trip, that is the relevant variable, not the linens.
- When should I get tested?
- A bed sheet does not start the testing clock; a real sexual exposure does. After that, test on the right window for the right infection: chlamydia or gonorrhea at about 14 days, syphilis at 6 weeks (retest at 3 months for high-risk exposures), HIV at 18 to 45 days for fourth-generation lab tests or 23 to 90 days for antibody-only home tests, HSV-2 antibodies at 12 to 16 weeks on most assays (a minority seroconvert by 6 to 8 weeks; an earlier negative should be repeated at 12 weeks), and hepatitis B or C antibodies at 8 to 12 weeks with a 6-month retest after high-risk exposures.
- Are at-home STI tests reliable?
- For screening purposes, yes. Rapid lateral-flow tests are accurate once you are past the window period for the specific infection. Two caveats apply: any positive is worth lab confirmation before treatment decisions, and a negative result before the window closes warrants a retest. Lab NAAT panels remain the analytical gold standard, while at-home rapid tests provide a practical and private first screening step.
- U.S. Centers for Disease Control and Prevention. About Sexually Transmitted Infections, primary transmission routes for STIs.
- U.S. Centers for Disease Control and Prevention. About Genital Herpes, including explicit guidance on HSV non-transmission via toilet seats, bedding, and shared objects.
- U.S. Centers for Disease Control and Prevention. About Pubic Lice, including the 24 to 48 hour off-host survival window and possible spread via clothing or bedding.
- U.S. Centers for Disease Control and Prevention. About Scabies, including the two-to-three-day off-host survival window for scabies mites away from human skin.
- World Health Organization. Sexually transmitted infections (STIs) fact sheet, transmission categories.
- NHS. Sexually transmitted infections (STIs), patient overview of transmission and testing pathways.
