
Published: November 2025 | Last updated: April 2026
The question that brought you here usually has a messier answer than people want. A clean ranking does exist, but real-world risk depends on at least five variables stacked together: the sex act itself, the specific infection, whether barriers were used correctly, where each partner sits in their own testing cycle, and whether anyone has visible symptoms or asymptomatic shedding. The ranking is useful, though the habits around it matter more.
This guide breaks down per-act risk for the three most-asked-about acts (oral, vaginal, anal), plus the harder-to-find data on rimming, shared toys, dry humping, and outercourse. Every numeric claim is sourced. The product recommendations are matched to what each act can plausibly transmit, not bolted on as an upsell.
Which sex act actually carries the highest STD risk?
Receptive anal sex has the highest per-act risk for HIV and several bacterial STIs, because rectal tissue is thin and easily microabraded. Receptive vaginal sex sits next, followed by oral sex on a penis. Oral sex is not the safe alternative many people assume: gonorrhea, syphilis, herpes, and chlamydia all transmit through it, and throat infections are usually asymptomatic. Skin-to-skin acts like dry humping carry the lowest risk, though HSV and HPV can still spread without penetration.
Why anatomy decides risk, not partner count
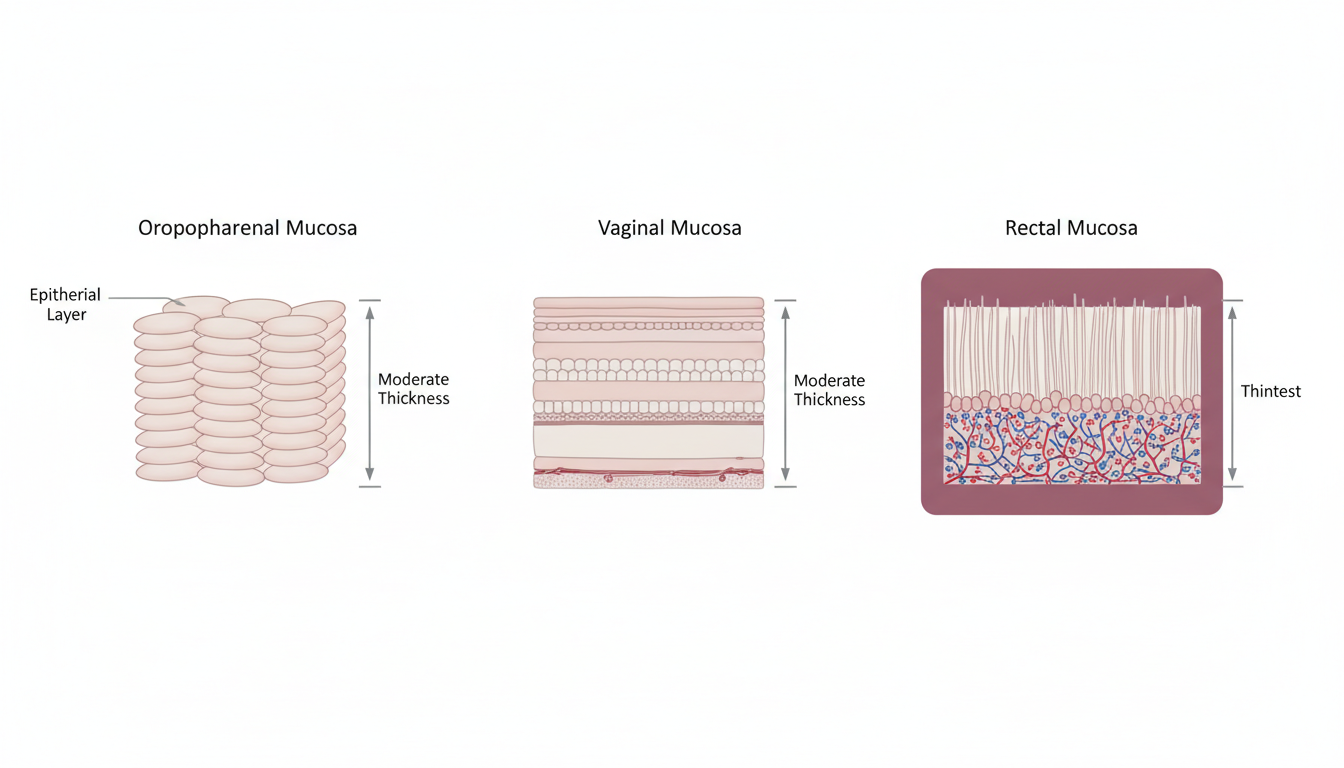
STD transmission is not a moral measurement. It tracks tissue biology, fluid exposure, and viral or bacterial load. The rectum is lined by a single layer of columnar epithelium, sits over a dense vascular bed, and produces no natural lubrication. That combination means tiny abrasions occur readily during receptive anal sex and offer a direct route into the bloodstream. The vaginal canal uses stratified squamous epithelium several cell layers thick and is more resilient. The oropharynx and oral mucosa are tougher again, but they still host receptors that gonococci, chlamydia, herpes simplex, and Treponema pallidum (the bacterium that causes syphilis) can colonize.
Fluid composition matters too. Semen, pre-ejaculate, vaginal secretions, and rectal mucus carry different concentrations of HIV when an infected partner is not on suppressive treatment. Saliva carries trace HIV but at concentrations that, in real-world studies, almost never produce transmission (CDC, About STI Risk and Oral Sex). Gonococcal bacteria, by contrast, thrive in the moist tissue of the throat and can persist there asymptomatically for weeks.
None of this means more partners automatically equals more disease. Two careful partners who use barriers and test regularly will accumulate less exposure than one partner who skips both. The ranking that follows applies per-act with no protection in place.
The risk ranking by sex act
Public health agencies and peer-reviewed transmission studies have produced consistent rankings of relative per-act risk. The table below assumes no protection is used, no antiretroviral therapy or PrEP is in play, and one partner is infected and untreated. Real risk in any specific encounter rises or falls with viral load, condom use, adequate lubrication, the partner's recent testing history, and whether either partner has visible lesions or asymptomatic shedding.
| Sex Act | Primary STDs Transmitted | Relative Per-Act Risk | Why It Sits Where It Does |
|---|---|---|---|
| Receptive anal sex | HIV, gonorrhea, chlamydia, syphilis, HPV, herpes | Very high | Thin rectal epithelium, dense vascularity, frequent microabrasions |
| Insertive anal sex | HIV, chlamydia, gonorrhea, syphilis | High | Exposure to infected rectal secretions; urethral entry |
| Receptive vaginal sex | Chlamydia, gonorrhea, trichomoniasis, HIV, HPV, herpes | Moderate to high | Cervical and vaginal mucosa exposure to semen and pre-ejaculate |
| Insertive vaginal sex | Chlamydia, gonorrhea, HIV, trichomoniasis | Moderate | Urethral exposure to vaginal secretions |
| Oral on penis (fellatio) | Gonorrhea, chlamydia, syphilis, herpes, HPV | Moderate | Pharyngeal exposure to urethral secretions; usually asymptomatic |
| Oral on vulva (cunnilingus) | Herpes, HPV, gonorrhea, syphilis | Lower to moderate | Oral mucosa contact with vaginal secretions and skin |
| Anilingus (rimming) | Hepatitis A, herpes, gonorrhea, intestinal parasites (Giardia, Entamoeba histolytica, Cryptosporidium) | Moderate | Fecal-oral route plus mucosal STD exposure |
| Shared sex toys (uncleaned, unbarriered) | Chlamydia, HPV, herpes, trichomoniasis | Moderate | Direct mucosal-to-mucosal pathogen transfer between partners |
| Dry humping or outercourse | HSV, HPV | Low (not zero) | Skin-to-skin contact; possible during shedding or visible lesions |
Why receptive anal sex sits at the top
The CDC's HIV risk modeling places receptive anal sex as the highest-risk sexual behavior for HIV transmission. Per-act risk is substantially higher than for insertive anal sex (HIV.gov, Preventing Sexual Transmission of HIV). The driver is anatomy, not orientation: the rectal lining is thin, lacks natural lubrication, and sits directly over a vascular bed. Microtears occur even when sex feels comfortable, and infectious fluid reaches the bloodstream more readily than at any other commonly exposed site.
Anal sex is not inherently unsafe. The math changes substantially when condoms are used correctly with adequate water-based or silicone lubrication, when the receptive partner is on PrEP, and when both partners screen extragenitally (rectal swabs, not just urine or genital tests). Many couples who include anal sex routinely have lower aggregate STD exposure than couples who assume vaginal-only sex is automatically safer and skip testing.
Extragenital screening is also frequently missing from a default STD panel; rectal chlamydia and gonorrhea slip past unless you specifically request a rectal swab. Ejaculation is also not required for transmission, since pre-ejaculate carries enough infectious viral or bacterial load to seed an infection, particularly with HIV and chlamydia.
Our at-home kits validate fingerstick blood and self-collected genital swabs only. Rectal swabs require a clinic. The HIV antibody test below is a useful baseline for anyone reassessing their risk, and the CDC recommends pairing it with full-site bacterial screening at a clinic if you have receptive anal sex with new or untested partners.

Oral sex is not the safe alternative
Oral sex gets dismissed as risk-free more often than any other act, and that assumption is the single biggest gap in self-managed sexual health. Gonorrhea, chlamydia, syphilis, and herpes simplex all transmit reliably through oral sex. HIV transmits rarely (saliva and the oral mucosal barrier reduce viability), but it is not zero (CDC, About STI Risk and Oral Sex).
The trickier reality is that oropharyngeal infections are usually silent. Pharyngeal gonorrhea produces a sore throat in a minority of cases; most carriers feel nothing and pass it on through subsequent oral sex. Pharyngeal chlamydia behaves similarly. The infections are still treatable, often with the same antibiotic regimens used for genital infection, but only after they are detected.
| STI | Transmits via Oral Sex? | Symptoms in Throat or Mouth? | How It Is Detected |
|---|---|---|---|
| Gonorrhea | Yes (commonly) | Usually none; occasional sore throat | Pharyngeal swab at a clinic; lab NAAT |
| Chlamydia | Yes (less efficient than genital) | Usually none | Pharyngeal swab at a clinic; lab NAAT |
| Syphilis | Yes | Painless sore (chancre) on lip, tongue, or throat in primary stage; later rash and systemic | Blood antibody test |
| Herpes (HSV-1, HSV-2) | Yes (cold-sore lesion to genitals or vice versa) | Cold sores around mouth or in throat; sometimes none | Lesion swab when active; blood IgG when no lesion |
| HPV | Yes (oropharyngeal HPV is a known oropharyngeal cancer risk) | Usually none until lesion or cancer develops | Not routinely tested; vaccination is the primary defense |
| HIV | Rarely | None from the oral route itself | Blood or oral fluid antibody/antigen test |
Our at-home rapid kits cover self-collected genital swabs and fingerstick blood draws. We do not sell pharyngeal (throat) or rectal swab tests. If your concern is throat-specific (sore throat after oral sex, or you want a clean read on pharyngeal gonorrhea), see a clinic and ask explicitly for an extragenital swab panel. Our genital chlamydia plus gonorrhea kit below covers the same-organism risk from genital exposure during the same encounter, which is often the more common follow-up question after a mixed-act night.

Vaginal sex and the assumption that it is the safe default
Vaginal sex sits in the middle of the per-act ranking, but it is the act that most often hides infections in long-term relationships. The reason is asymptomatic carriage. Chlamydia, gonorrhea, and trichomoniasis can all persist for months in the vaginal canal, urethra, or cervix without symptoms. People with vulvas may experience subtle changes that get pattern-matched to a yeast infection. People with penises may have no symptoms at all, even while shedding the same organism in their urethral secretions.
Trichomoniasis is the most underdiagnosed of the three. It is the most common curable non-viral STI worldwide and is frequently picked up incidentally on a routine pap smear in someone who had assumed they were free of infection (WHO, STI fact sheet). Long-term partners often discover it after a years-long gap with no testing.
Condoms reduce transmission for fluid-borne infections substantially when used correctly across the entire act. The reduction is not 100 percent. Condoms do not cover the base of the penis, the mons pubis, or the upper thighs, which means HSV-2 lesions and HPV warts in those areas can still transmit during vaginal sex with a condom in place.
Practical move for anyone in a longer relationship who has not tested in over a year: a baseline panel covering chlamydia, gonorrhea, trichomoniasis (women), HIV, and syphilis catches most of the asymptomatic gaps. Add a herpes blood IgG only if you have a specific concern (the IgG result is meaningful only as confirmation of past exposure, not a current outbreak).
WHO data report roughly 156 million new trichomoniasis infections, 129 million chlamydia, and 82 million gonorrhea cases globally each year. The majority of these infections are asymptomatic at the time of transmission, which is why routine screening matters even in long-term relationships where neither partner has noticed anything wrong.
Outercourse, dry humping, and the lowest-risk acts still have caveats
Genital touching, dry humping, mutual masturbation, and most forms of outercourse sit at the bottom of the per-act risk list. They are not zero. HSV and HPV both transmit through skin-to-skin contact, and that contact does not require penetration. A partner who is shedding HSV asymptomatically can transmit through close genital-to-genital contact, even through thin fabric, though the per-act probability is low.
Hepatitis B can transmit through any exposure to infected blood or genital secretions, which means broken skin or visible lesions during fingering or fisting, particularly without gloves, can carry risk. Vaccination for hepatitis B is the highest-leverage prevention move here, since the vaccine is highly effective and durable.
Outercourse meaningfully reduces but does not eliminate risk for HSV, HPV, and (rarely) hepatitis B. It eliminates almost all risk for HIV, chlamydia, gonorrhea, and trichomoniasis, since those organisms need fluid-borne or mucosal transmission routes that outercourse generally does not provide.
Essentially eliminated: HIV, chlamydia, gonorrhea, and trichomoniasis (these need fluid-borne or mucosal transmission routes). Only reduced, not eliminated: HSV and HPV (both spread through skin-to-skin contact even through thin fabric) and rarely hepatitis B (when blood or genital secretions reach broken skin).
Shared toys, group play, and the management problem
The risks that catch people off-guard during group sex or extended play sessions usually centre on fluid management and shared objects rather than the acts themselves. A shared dildo or vibrator that moves between partners without a barrier change, or without cleaning, is functionally a third partner from a transmission standpoint. Chlamydia, gonorrhea, trichomoniasis, HPV, and herpes can all transfer this way.
Habits that close most of this gap:
- Put a fresh condom on a toy before each new partner uses it. The condom is the barrier; switching is the protection.
- Use medical-grade nitrile gloves for fingering or fisting if cuts, hangnails, or trimmed-too-short cuticles are in play, or if either partner has menstrual blood or anal exposure. Gloves prevent the bidirectional fluid exchange that fingering can otherwise become.
- Get the hepatitis A vaccine if rimming is a regular part of your sex life. Hepatitis A transmits via fecal-oral exposure, the vaccine is durable, and the disease is otherwise unpleasant for weeks.
Open communication about who is on PrEP, who has tested recently, and which barriers stay on through which transitions is more protective than any single product. A setting that feels too rushed for those conversations is worth slowing down or stepping away from.
Wash silicone or hard-plastic toys with soap and warm water between uses. Boilable silicone toys can be sterilised by 5 minutes in boiling water between sessions. Porous materials (jelly, TPE, latex) cannot be fully sterilised; always cover them with a fresh condom for each new partner and replace toys made of these materials more frequently.
Where condoms protect, and where they do not
Condoms are the single most effective barrier method for fluid-borne STIs. They reduce HIV transmission by upwards of 90 percent with consistent and correct use, and they cut chlamydia, gonorrhea, and trichomoniasis transmission substantially as well. They are imperfect against any infection that spreads through skin contact outside the area the condom covers.
Two practical fixes close most of the gap condoms leave: pair condoms with regular testing for all sexually active partners, and consider HSV and HPV-specific behaviors (avoid sex during a visible HSV outbreak, get the HPV vaccine if eligible).
| Infection | Transmission Mode | Condom Effectiveness | Why |
|---|---|---|---|
| HIV | Bloodborne, fluid-borne | Highly effective | Latex blocks viral particles in semen and vaginal secretions |
| Chlamydia | Fluid-borne (urethral, cervical) | Highly effective with correct use | Urethral and cervical secretions contained by the condom |
| Gonorrhea (genital) | Fluid-borne | Highly effective | Same fluid-blocking mechanism |
| Trichomoniasis | Fluid-borne | Effective | Vaginal secretions contained |
| Syphilis | Lesion contact (chancre) | Partial | Chancres can occur on areas a condom does not cover (scrotum, mons, mouth) |
| Herpes (HSV-1, HSV-2) | Skin-to-skin | Partial | Lesions and asymptomatic shedding occur on skin outside the condom |
| HPV | Skin-to-skin | Partial | Same: skin contact at the base of the penis or vulva is uncovered |
| Hepatitis B | Bloodborne, fluid-borne | Effective; vaccine is the main defense | Vaccine durably prevents infection regardless of barrier failure |
When to test after potential exposure
The window period (the time between exposure and when an infection reliably shows up on a test) varies by infection and by test technology. Testing too early is a common reason for false-negative results that delay treatment. The CDC's testing guidance and the FDA-approved labels for at-home rapid tests both publish these windows; they are not arbitrary.
For most people after a single recent exposure, the practical pattern is to test once at the earliest reliable window for the infections you are most concerned about, then retest at 12 weeks for the slower-seroconverting infections (HSV blood IgG, hepatitis C). If post-exposure prophylaxis (PEP) for HIV is on the table, the decision window is 72 hours from exposure, and that is a clinic visit, not a self-managed step (HIV.gov, sexual transmission prevention).
| Infection | Earliest Reliable Test Window | Notes |
|---|---|---|
| Chlamydia | From 14 days after exposure | Genital swab or urine; lab NAAT remains the gold standard |
| Gonorrhea | From 14 days after exposure | Genital swab; pharyngeal and rectal swabs require a clinic |
| Trichomoniasis | 7 to 14 days after exposure | Vaginal self-swab; women only for at-home rapid |
| Syphilis | 3 to 6 weeks after exposure for blood antibody | Earlier dark-field microscopy possible only if a chancre is present |
| HIV (Ag/Ab lab combo) | From 18 to 45 days | Fourth-generation lab test; earlier than antibody-only |
| HIV (rapid antibody) | From 23 to 90 days | At-home rapid blood test; window is longer than lab combo |
| Herpes (HSV) blood IgG | 12 to 16 weeks for reliable seroconversion | Active lesion swab is more accurate during an outbreak |
| Hepatitis B (surface antigen) | From 4 weeks; up to 9 weeks | Vaccination history matters for interpretation |
| Hepatitis C (antibody) | From 8 to 11 weeks; up to 6 months | RNA test detects earlier |
Anal sex is the highest-risk sexual behavior for HIV transmission. Receptive anal sex is much riskier than insertive anal sex.
A practical move: test, then plan
The single most useful thing you can do after any encounter that you are second-guessing is to write down the date and the act, then look up the right window for the infections that act can transmit. Test once at the early-end window, plan a follow-up at the late-end window, and treat anything in between as preliminary. This is how clinicians manage exposure follow-ups, and it works just as well at home with the right kit.
For mixed-act encounters where multiple infections are plausibly in play, a multi-infection panel saves the cost and friction of running several single tests in sequence.

Frequently asked questions
- Can you actually get an STD from oral sex?
- The assumption that oral sex is low-risk is the single most widespread gap in sexual-health self-management. Gonorrhea and chlamydia are common in the throat after fellatio; syphilis transmits through any mucosal contact including the lips and tongue; herpes (particularly HSV-1) is the most efficiently transmitted of the group. HIV is the exception, with salivary transmission theoretically possible but clinically rare. Throat-specific testing requires a clinic swab; at-home rapid kits are validated for genital and bloodwork sample types.
- Is anal sex automatically dangerous?
- Receptive anal sex carries the highest per-act risk for HIV among common sexual behaviors, per CDC modeling. The risk drops substantially with consistent condom use, adequate water-based or silicone lubrication, and PrEP for the receptive partner. Couples who include anal sex routinely and test extragenitally often have lower aggregate exposure than couples who treat vaginal-only sex as safe and skip testing.
- Do condoms block every STD?
- Condoms are highly effective for fluid-borne infections (HIV, chlamydia, gonorrhea, trichomoniasis). They are partial protection against skin-to-skin infections (HSV, HPV, syphilis chancres) because lesions and shedding can occur on skin the condom does not cover. Pair condoms with regular testing and the HPV vaccine for the most complete coverage.
- How soon after sex can I test?
- The honest answer depends on the infection. Chlamydia and gonorrhea are reliably testable from day 14. Syphilis blood antibody is reliable from 3 to 6 weeks. HIV via at-home rapid antibody test is reliable from 23 to 90 days; lab Ag/Ab combo is faster (18 to 45 days). HSV blood IgG needs 12 to 16 weeks. Test at the early end of the window for the infections you are most worried about, retest at the late end, and treat anything in between as preliminary.
- What if my partner says they are clean?
- The word clean is medically meaningless. Most people who carry an asymptomatic STI feel completely fine. Unless your partner has been tested recently and at every relevant site (genital, throat, rectum where applicable), they may not know their actual status. Asking when and what they were tested for is a more useful conversation than asking whether they are clean.
- Does pre-ejaculate carry STDs?
- Yes. Pre-ejaculate carries enough viral or bacterial load to transmit HIV, chlamydia, and gonorrhea. The pull-out method is not a meaningful barrier for STD prevention (it is also a poor contraception method). Condoms used from start to finish are the appropriate barrier.
- Is dry humping or outercourse risk-free?
- Lower risk, not zero risk. HSV and HPV both transmit through skin-to-skin contact, including through thin fabric, particularly when one partner is shedding asymptomatically. Outercourse essentially eliminates risk for HIV, chlamydia, gonorrhea, and trichomoniasis, because those infections need mucosal or fluid-borne transmission.
- Can I test my throat or rectum at home?
- Not with our kits, no. Our at-home rapid tests are validated for self-collected genital swabs (chlamydia, gonorrhea, trichomoniasis, HPV) and for fingerstick blood draws (HIV, syphilis, HSV-1, HSV-2, hepatitis B, hepatitis C). Pharyngeal and rectal swabs require a clinic, where the lab uses NAAT (molecular) testing. If your concern is specifically a throat or rectal infection, book a clinic visit and ask explicitly for an extragenital swab panel; otherwise it will not be included by default.
- U.S. Centers for Disease Control and Prevention. About STI Risk and Oral Sex (transmissible STIs through oral sex, asymptomatic carriage in the throat).
- HIV.gov. Preventing Sexual Transmission of HIV (per-act risk by sexual behavior, role of PrEP, PEP timing, anal sex as highest-risk behavior).
- U.S. Centers for Disease Control and Prevention. Sexually Transmitted Infections Treatment Guidelines (testing windows, screening recommendations, extragenital site screening).
- World Health Organization. Sexually transmitted infections fact sheet (global epidemiology, trichomoniasis as the most common curable non-viral STI, asymptomatic-carriage prevalence).
- National Institutes of Health, MedlinePlus. Sexually Transmitted Diseases overview (clinical context for asymptomatic carriage and symptom variability across common STIs).
- UK National Health Service. Sexually transmitted infections (testing access, condom protection, partner notification).
