
Published: April 2025 | Last updated: May 2026
For a long stretch of the HIV epidemic, getting tested meant a clinic visit, a paper form, and a few uncomfortable days between the blood draw and the call. That model still exists, and for many situations it is still the right one. Beside it now sits something newer: a small lateral-flow test you can run at home in roughly 20 minutes, on a sample you collect yourself. The U.S. CDC's HIV testing page lists self-testing as one option among rapid, lab, and clinic-based tests, and points readers to gettested.cdc.gov for free or low-cost kits.
The technology has been on the U.S. market since the FDA cleared the first over-the-counter OraQuick In-Home HIV Test in July 2012. What changed is how widely people use it. Free programs like the CDC-backed Together TakeMeHome now mail kits to U.S. addresses on a 90-day cadence, and the World Health Organization helped negotiate a one-dollar price point for WHO-prequalified self-tests in low- and middle-income countries. The question now is less “do these tests exist?” and more “which test, at what point in time, in what circumstance?” This explainer walks through what an at-home HIV kit can answer, where it falls short, and what is moving through the diagnostic pipeline for the next few years.
From a clinic appointment to a kitchen counter
Stigma has historically been the biggest barrier to HIV testing in the U.S. and globally, not cost or access alone. The World Health Organization's HIV/AIDS fact sheet notes that fear of being seen at a clinic, fear of an unsupportive provider, and fear of inadvertent disclosure to family or community members all push people away from clinic-based testing. The pattern is especially pronounced among men who have sex with men, transgender people, and sex workers in countries where their identities carry legal or social risk.
At-home testing changes the geometry of that decision. The test arrives in a discreet box, the sample is taken in private, and the result is read in under half an hour by the person whose result it is. In WHO pilot programs across multiple regions, people offered a choice between facility-based and self-testing have repeatedly chosen self-testing in significant numbers, including many who had not tested in years or at all.
Regulatory work, distribution scaling, and the COVID-era normalization of home diagnostics have together moved at-home testing from a niche option to a mainstream one over the past five years. The WHO's 2022 price negotiation brought one prequalified self-test within reach of public-sector programs in low- and middle-income countries. The U.S. Together TakeMeHome program ships free kits on a 90-day cadence, and the NHS in the UK includes home testing alongside clinic-based options for residents who request it. COVID-19 normalized at-home diagnostics across the board, from pregnancy tests to PCR collection kits, reducing the cultural distance between “swabbing yourself” and “going to the doctor.”
In the U.S., the CDC-backed Together TakeMeHome program mails free OraQuick In-Home kits to eligible residents on a roughly 90-day cadence; orders go through gettested.cdc.gov. In the UK, the NHS offers free home testing in many regions through local sexual-health services. Internationally, WHO-prequalified self-tests have been available through public-sector channels for around one US dollar in participating countries since the 2022 price negotiation.
What's actually in an at-home HIV kit
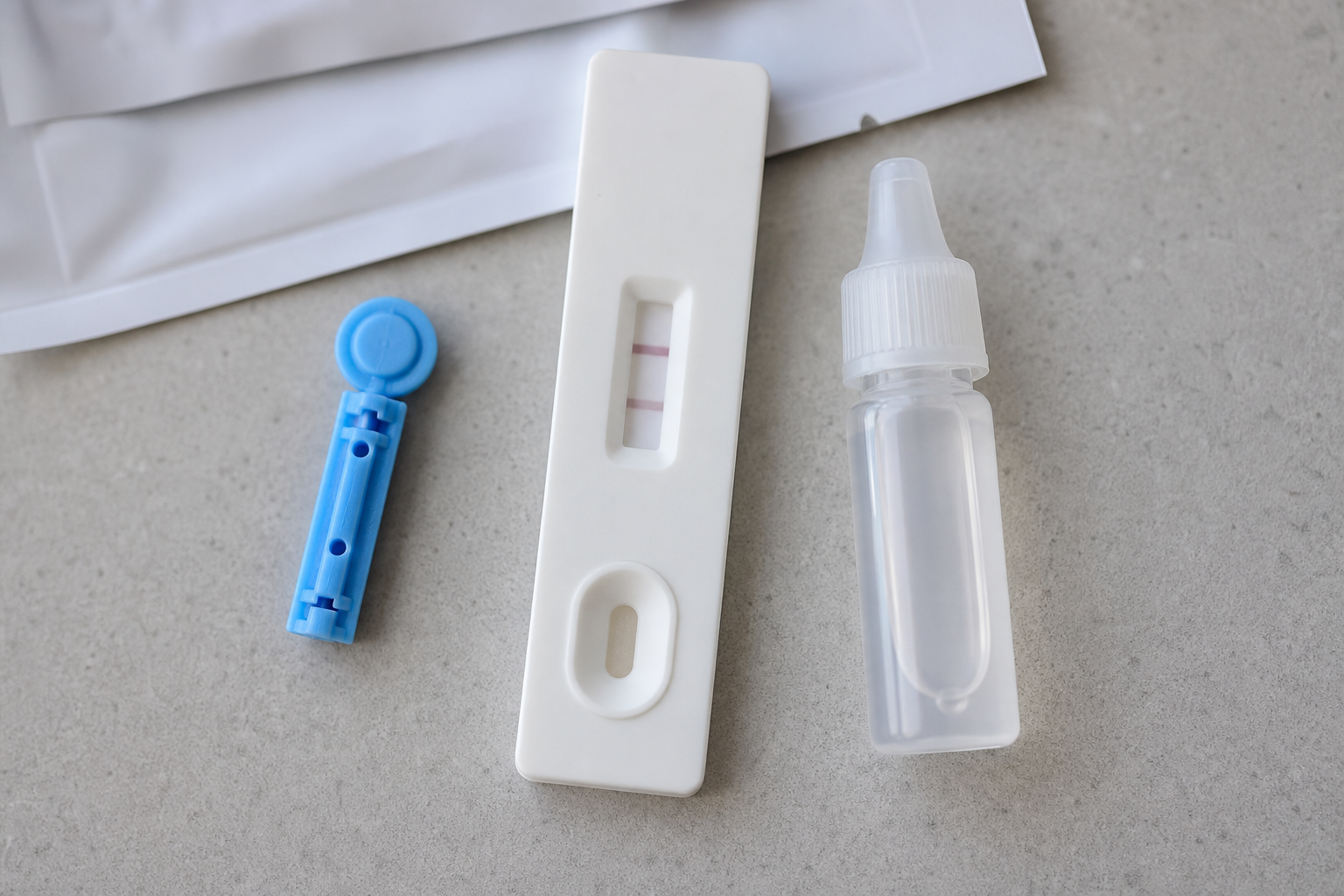
Most consumer-facing at-home HIV tests work on one of two sample types: oral fluid swabbed from the gum line, or a small drop of blood from a fingerstick. Both are lateral-flow immunoassays, the same general format as a home pregnancy test. The kit contains a plastic cassette with a strip of absorbent paper inside it, a developer or buffer solution, a sample-collection device (a soft pad on a stick for oral fluid, or a small lancet plus collection well for blood), and a printed set of instructions. The active chemistry on the strip is a band of immobilized antigens that will bind to HIV antibodies if any are present in the sample.
When the sample plus buffer flows along the strip, antibodies, if present, stick to the antigen band and trigger a visible colored line: the test band. A second built-in control band confirms the test ran correctly. Two visible lines mean reactive (often labeled “preliminary positive”). One control line alone means non-reactive. No control line means the test is invalid and the kit was wasted, which is part of why instruction clarity has become a bigger focus for newer kits.
A critical distinction: antibody-based home tests look for the body's immune response to HIV, not the virus itself. That response takes time to develop, which is what creates the “window period” discussed in the next section. Laboratory NAAT (nucleic acid amplification testing) and fourth-generation antigen-antibody tests, both performed by labs rather than at home, can detect HIV earlier because they look for either the virus's genetic material or its p24 antigen (a viral protein that appears in the bloodstream before antibodies develop) directly. Lateral-flow at-home tests and lab NAATs are not equivalent technologies; they are complementary. Home tests are fast, private, and accessible for first-line screening. Lab tests are the gold standard for confirmation and for catching very recent infections.
A final note on what this site sells. Our HIV rapid kit (single-infection) is a fingerstick blood antibody test, not an oral swab. The wider combination kits add other blood and swab-based panels alongside the HIV blood antibody strip.
Accuracy, window periods, and the math behind a negative result
“Accuracy” is the most asked question about at-home HIV testing, and also the most often miscommunicated. The honest answer comes in two parts.
First, the laboratory accuracy of the test in ideal conditions, expressed as sensitivity (true positives the test catches) and specificity (true negatives the test correctly identifies). The original OraQuick In-Home HIV Test was cleared by the FDA in July 2012 with a measured sensitivity of roughly 93% and a specificity of about 99.98% in untrained home-user trials, somewhat lower sensitivity than the same chemistry used by trained clinicians. Second- and third-generation lateral-flow self-tests report higher figures: the INSTI HIV Self Test and the autotest VIH have published sensitivity and specificity of 99.7 to 99.8% in healthcare-worker-administered studies per Aidsmap's review of the published evidence. Lay-user performance at home is somewhat lower: the same review found that roughly 97 to 98% of lay users obtained a valid result when running the tests themselves, with higher invalid-result rates on blood-based kits than on oral-fluid ones. All of these figures assume the test is run outside the window period.
That second part is the larger story. The CDC publishes the following window-period ranges by test technology: antibody tests (the at-home category) can usually detect HIV 23 to 90 days after exposure; rapid antigen/antibody tests, 18 to 90 days; antigen/antibody lab tests, 18 to 45 days; and lab NAAT, 10 to 33 days. Inside those windows, a test can return a negative result even though infection is present, because the body has not yet produced enough antibody to trigger the test band. A three-week-post-exposure negative on an at-home antibody test is reassuring but not definitive, and the CDC recommends a re-test at or after the upper bound of the window if the exposure carried meaningful risk.
Practical translation:
- Test now if you want a baseline reading and have had no high-risk exposure in the past 90 days.
- If you have had a high-risk exposure, test now for a baseline plus a re-test at the 90-day mark for at-home antibody kits. Earlier results inside the window period are not definitive.
- If a possible exposure is very recent (within the last 72 hours) and the risk was high, talk to a clinician about post-exposure prophylaxis (PEP) rather than waiting on a self-test result. PEP is time-sensitive.
A negative test outside the window is a strong screening result. A positive test, by FDA labeling and by every guideline body (CDC, WHO, NHS), is a preliminary positive that requires laboratory confirmation. False-positive rates on lateral-flow self-tests are low but not zero, which is exactly why confirmation matters: it protects people from acting on a result that turns out to be a strip artifact.
How accurate are at-home HIV tests?
FDA-cleared lateral-flow self-tests have published sensitivities ranging from about 93% (the original OraQuick In-Home) to roughly 99.8% on newer second- and third-generation devices in healthcare-worker-administered studies, with specificity above 99% across the category. Lay-user performance at home runs somewhat lower, with invalid results on roughly 2 to 3% of attempts in the Aidsmap review. CDC guidance is that antibody-based home tests are most reliable 23 to 90 days after a possible exposure. Inside that window, a negative result is not definitive and should be retested. A positive result, in any window, is a preliminary positive that needs laboratory confirmation.
Where at-home HIV tests are the wrong tool
Self-testing is a powerful screening layer that public-health programs broadly agree is still under-used. It is also not the right answer in every situation. A short list of scenarios where a clinic visit beats an at-home strip:
Very recent exposure (under 72 hours). PEP, a 28-day antiretroviral regimen taken after a high-risk exposure, can dramatically reduce the chance of seroconversion when started within 72 hours. PEP is prescription-only and time-critical. Waiting on a self-test result here trades time for nothing useful, because no test on the market will reliably show seroconversion this early in the window.
Starting pre-exposure prophylaxis (PrEP). Initiating PrEP requires a baseline HIV-negative status documented by a clinician, plus kidney function and STI screening that no home test offers. Ongoing PrEP also requires periodic clinic-based testing per CDC PrEP guidelines. Home tests can complement, but not replace, that workflow.
Confirmation after a reactive home test. Every reactive self-test needs lab confirmation. This is not a sales pitch for clinic testing; it is what FDA labeling, CDC, WHO, and NHS guidance all explicitly require. A confirmed diagnosis is also the entry point into antiretroviral therapy, which today can take someone from diagnosis to an undetectable viral load in a matter of months.
Suspected acute (early) HIV infection with symptoms. Fever, rash, sore throat, swollen lymph nodes, and night sweats in the two-to-four weeks after a high-risk exposure can indicate acute HIV. At that stage, lab NAAT or a fourth-generation antigen-antibody test is the right tool, because antibody-only home tests are likely to be falsely negative inside the window.
Each of those four scenarios is a reason to book a clinic visit rather than reach for a home kit.
Post-exposure prophylaxis (PEP) is a 28-day antiretroviral regimen that can dramatically reduce the chance of HIV seroconversion when started within 72 hours of a high-risk exposure. PEP is prescription-only and time-critical. Contact a clinic, urgent care, or an emergency department about PEP rather than waiting on a self-test result, because no at-home antibody test will reliably show a very recent infection inside the window period.

What's next: CRISPR detection, multiplex panels, and connected follow-up
CRISPR-based diagnostics are the most-watched development on the horizon. They use programmable molecular scissors to recognize specific viral genetic sequences directly, rather than waiting for an antibody response. Early-stage work on at-home CRISPR HIV detection aims to shrink the window period from the 23-to-90-day antibody range toward the 10-to-33-day NAAT range, without requiring a laboratory. The technology is moving, but no FDA-cleared at-home CRISPR HIV test exists on the consumer market yet. Treat any “CRISPR home HIV test” marketing claim with caution until the FDA labeling is in hand.
Multiplex testing runs in parallel: a single sample (typically a few drops of fingerstick blood, or a swab) yielding results for multiple infections at once. Lateral-flow strips with multiple test bands, one per analyte, are the most straightforward design, and combined HIV-plus-syphilis-plus-hepatitis panels are already in clinical use in several countries. Several of the combination kits on this site use the same general approach for at-home screening across multiple infections in a single sitting.
Connected follow-up is the third and most active area of development. The hardest part of self-testing has never been the strip; it has been what happens next. App-based kits that walk the user through sample collection, time the result window, photograph the strip for AI-assisted line reading, and route reactive results to a telehealth provider for confirmation and care linkage are the most active area of development heading into 2026. Whether they replace clinic visits or simply make the path from positive screen to treatment smoother depends on regulatory work that is still in progress in most jurisdictions.
The trajectory is real, but the timeline is multi-year for any of these technologies to clear regulators and reach pharmacy shelves.
Several research groups are working on CRISPR-based at-home HIV detection, but as of 2026 no such device has cleared the FDA for over-the-counter use. If you encounter marketing copy claiming a “CRISPR home HIV test,” check the FDA labeling before relying on it. Until then, the at-home category is still antibody-based lateral-flow strips with the 23-to-90-day window discussed above.
A practical playbook: choosing a test for the moment
Different situations call for different tests. A simplified decision framework, drawing on CDC, WHO, and NHS guidance:
Routine annual baseline, no specific high-risk exposure in the past 90 days. An at-home antibody self-test is well-suited here. Pick a single-infection HIV kit if HIV is your only concern, or a combination kit if you also want screens for syphilis, hepatitis B, hepatitis C, plus chlamydia and gonorrhea swabs in the same sitting.
Possible exposure 4 to 12 weeks ago, not yet tested. Run an at-home antibody test now, and plan a re-test at the 90-day mark. A negative result before day 90 is reassuring but not definitive on antibody-based home tests; the second test inside the same time frame closes the window-period gap.
High-risk exposure in the past 72 hours. A home test is the wrong tool. Contact a clinic, urgent care, or emergency department about PEP, then return to home or clinic-based testing on the schedule your clinician recommends.
Starting or maintaining PrEP. Use the clinic-based testing that the PrEP regimen requires (baseline HIV-negative documentation, kidney function, STI panel). At-home tests do not substitute for that work, though some people use them as additional checks between scheduled clinic visits.
Long-term partnership, considering changing safer-sex practices. A pair of at-home tests taken together by both partners, with full window-period awareness, is one of the more useful applications of the technology. The same logic applies before starting any new sexual relationship where you want a shared baseline.
Reactive (positive) result on a home test. Take a screenshot or photograph of the result for your own records, then book a clinic confirmation. Modern treatment can take someone from a confirmed positive to an undetectable viral load (which, per the Undetectable = Untransmittable, or U=U, consensus, also means the virus cannot be passed to sexual partners) in a matter of months.

Bottom line
At-home HIV testing has earned its place in the screening toolkit. It is private, affordable, and accessible in ways that clinic testing has historically not been, and free-distribution programs have removed price as a meaningful barrier for many U.S. and UK residents. It is also a screening tool, with the diagnosis coming from a follow-up lab test: reactive results need confirmation, negative results need to respect the antibody window period, and recent high-risk exposures are still the right reason to call a clinic about PEP rather than to wait on a strip.
The next few years will bring faster detection chemistry, multiplex panels, and better app-mediated follow-up. None of those replace the fundamental discipline of testing on a sensible schedule and confirming reactive results in a lab. Used within those limits, an at-home HIV test is one of the more useful public-health tools to reach a kitchen counter in the past decade.
No HIV test can detect HIV immediately after infection.
FAQs
- How long after a possible exposure should I wait to take an at-home HIV test?
- For antibody-based at-home tests (the FDA-cleared home category), CDC guidance recommends 23 to 90 days after exposure for a reliable negative. A test inside that window can return a false negative because antibodies have not yet built up. If you have had a high-risk exposure, test now for a baseline and plan a re-test at the 90-day mark.
- Are at-home HIV tests as accurate as clinic tests?
- No, but the gap is smaller than most people assume. Laboratory NAAT and fourth-generation antigen-antibody tests are the diagnostic standard, particularly for confirming reactive results and detecting very recent infections. Home antibody-based tests are screening tools whose lay-user performance is somewhat lower than the same chemistry run by a clinician; the body of this article walks through the specific sensitivity figures and the healthcare-worker-versus-lay-user caveat from the Aidsmap review.
- What should I do if my home test is reactive (positive)?
- Treat it as a preliminary positive that needs laboratory confirmation, not a final diagnosis. Book a clinic confirmation as soon as you can. Modern HIV treatment, started promptly, can bring viral load to undetectable (and per the U=U consensus, non-transmissible) levels within months.
- Can a home test detect very early or acute HIV?
- Antibody-based home tests generally cannot reliably detect HIV in the first two to four weeks after exposure. If you have flu-like symptoms (fever, rash, sore throat, swollen lymph nodes) within that window of a high-risk exposure, ask a clinician about lab NAAT, which can detect HIV roughly 10 to 33 days after exposure.
- Are at-home HIV tests available for free?
- In the U.S., the CDC-backed Together TakeMeHome program mails free OraQuick In-Home kits on a roughly 90-day cadence to eligible residents who order through gettested.cdc.gov. In the UK, the NHS offers free home testing programs in many regions. Internationally, WHO-prequalified self-tests have been available through public-sector channels for around one US dollar in participating countries since the 2022 price negotiation.
- I'm on PrEP. Should I still use an at-home test between clinic visits?
- Home tests do not replace the clinic-based testing schedule that PrEP requires (baseline HIV-negative documentation, kidney function, periodic STI screening). Some people use home tests as an extra layer between scheduled clinic visits, but the regimen's clinic schedule is what protects the integrity of the PrEP workflow. Talk to your PrEP provider before changing your testing pattern.
- Does this site sell a throat or rectal swab HIV test?
- No. Our HIV rapid kit is a fingerstick blood antibody test. Pharyngeal (throat) and rectal swabs are clinically relevant for other STIs more than for HIV itself, and they are run on laboratory NAAT rather than at-home lateral flow. See a clinic if you specifically need those sample types.
- U.S. Centers for Disease Control and Prevention. HIV testing overview, including window-period ranges by test type and self-test ordering through gettested.cdc.gov.
- World Health Organization. HIV/AIDS fact sheet, including self-testing guidance and the requirement for confirmatory testing after a reactive screen.
- World Health Organization. New one-dollar price for WHO-prequalified HIV self-tests in low- and middle-income countries (July 2022 announcement).
- National Health Service (UK). HIV and AIDS overview, including home testing kit guidance and CE-marking requirements.
- Aidsmap. Accuracy review of HIV self-tests, including healthcare-worker-administered sensitivity and specificity figures and lay-user valid-result rates for OraQuick In-Home, INSTI HIV Self Test, and autotest VIH.
- U.S. Centers for Disease Control and Prevention. HIV program landing page, including links to testing, prevention (PrEP, PEP), and care resources.
