Published: July 2025 | Last updated: May 2026
Ten years ago, getting tested for an STI usually meant rearranging your day, sitting in a public clinic, and explaining your sex life to a stranger at the front desk. The barriers worked exactly as you would expect: people who needed testing the most often skipped it. Today, a small box arrives at your door in plain packaging, you collect a swab or fingerstick at home, and you get a real result within hours or days. The technology is genuinely good. The catch is that not all kits work the same way, and the question "is it reliable?" depends entirely on what kind of kit you are holding.
This article walks through what at-home STD kits measure, how their accuracy compares with a clinic visit, where they break down, and how to choose the right one for your situation. Where we cite a number, we name the source and the limit of what that number means.
Are at-home STD kits actually reliable?
Yes, when matched to the right job. Lab-processed mail-in kits use the same NAAT and antigen-antibody assays as clinic labs and report sensitivity in the mid-to-high 90s for most infections at the right time. Rapid at-home lateral-flow kits trade some lab-grade sensitivity for a 15-minute home result; treat them as a screening step and confirm any positive at a clinical lab before starting treatment. Window-period timing and correct sample collection matter more than brand.
What Counts as a Reliable Home STD Test?
"Reliable" sounds simple, but in lab medicine it has two technical pieces. Sensitivity is the percentage of true infections the test correctly identifies (a sensitivity of 97% means the test catches 97 out of 100 actual positives). Specificity is the percentage of uninfected people the test correctly clears (a specificity of 99% means only 1 in 100 uninfected people gets a false positive). "Accuracy" by itself is imprecise: a test can be highly accurate by averaging the two and still miss a meaningful number of real infections.
The U.S. FDA reviews home-use diagnostic tests for both numbers before they reach the market, and FDA-cleared kits publish their performance data on the package insert and product page. When you compare home kits, the figure to look for is the published sensitivity and specificity for the specific infection, not a generic "99% accurate" marketing line.
There are two practical categories of at-home STD kit, and they live in different parts of the accuracy curve:
- Lab-mailed kits: you collect a sample at home (swab, urine, fingerstick blood) and ship it to a CLIA-certified laboratory. The lab runs the same NAAT (nucleic acid amplification test) for chlamydia and gonorrhea, the same fourth-generation antigen-antibody combo for HIV, and the same RPR or treponemal test for syphilis that a hospital lab would run. Performance lives in the mid-to-high 90s for sensitivity and specificity for most infections, per the CDC's screening recommendations.
- Rapid at-home lateral-flow kits: you collect a sample, run it on a cassette at home, and read a test line in 10 to 20 minutes. Lateral-flow chemistry is faster and simpler, but the analytical sensitivity is lower than a lab NAAT. These kits are useful for screening (catching the obvious cases quickly and privately), and any positive should be confirmed with a lab test before treatment.
FDA clearance means the manufacturer submitted clinical performance data showing the home version of the test agrees with a reference lab method to a defined accuracy. CLIA certification is a separate signal that the lab itself meets federal standards for running the assay. A reputable home STI kit checks both boxes: an FDA-cleared device, processed (if mail-in) by a CLIA-certified lab.
Lab-Mail vs Rapid Home Tests: Two Different Technologies
The single biggest source of confusion in this space is treating "home test" as one product. Mail-in and rapid kits are different technologies with different jobs.
Mail-in lab kits ship to a CLIA-certified facility that runs molecular tests (NAATs for chlamydia and gonorrhea, qualitative PCR or antigen-antibody for HIV, RPR plus a treponemal confirmatory for syphilis). NAAT is the gold-standard reference method for bacterial STIs, per CDC laboratory guidance. Self-collected vaginal swabs perform comparably to clinician-collected swabs for chlamydia and gonorrhea, which is why mail-in kits work as well as a clinic visit when the swab is taken correctly.
Result turnaround is typically 2 to 5 business days after the lab receives your sample. The trade-off is that you are shipping biological material, so timing assumes the courier and lab run smoothly.
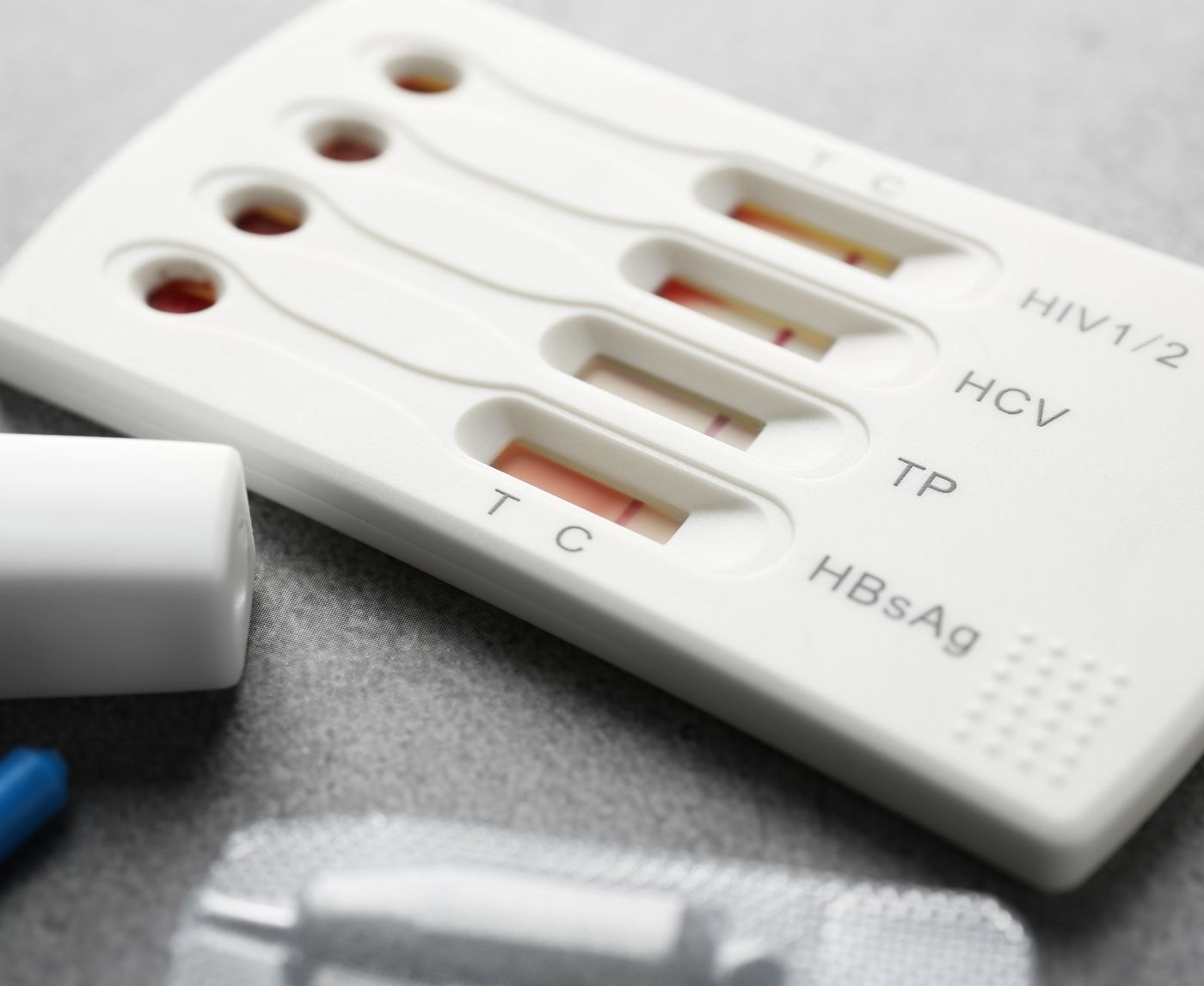
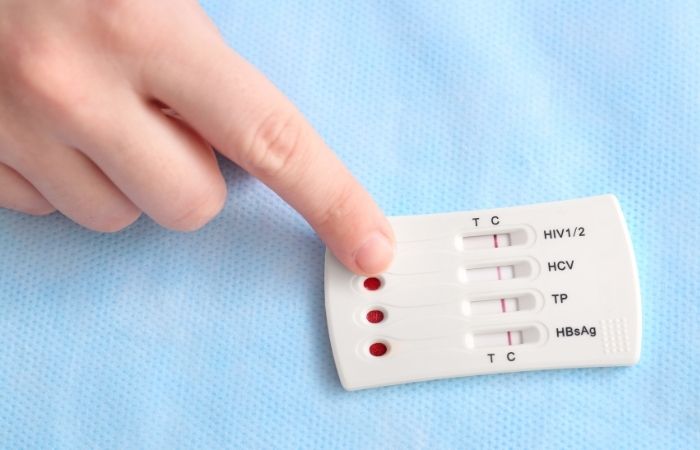
Rapid at-home lateral-flow kits are immunoassays that you read yourself on a cassette, the same technology as a home pregnancy test or a COVID-19 rapid antigen test. They detect antibodies (HIV, HSV, syphilis treponemal antibody, hepatitis) or antigens (chlamydia, gonorrhea protein) directly on the strip. The chemistry is fast (about 15 minutes) and private, but the limit of detection is higher than a lab NAAT, so the test needs a higher microbial load before it turns positive.
What this means in practice: a lateral-flow rapid test will correctly identify most established infections, but it can miss very early or very low-level cases that a lab NAAT would catch. Lateral-flow chemistry trades some lab-grade sensitivity for speed and simplicity by design. The right way to think about a rapid kit is as a high-utility screening tool: it tells you quickly whether you almost certainly need to act, and a positive result should be confirmed with a lab method before starting any treatment.
| Feature | Lab-mailed home kit | Rapid at-home lateral-flow kit |
|---|---|---|
| Test method | NAAT, antigen-antibody, RPR (lab) | Lateral-flow immunoassay (cassette) |
| Sample type | Self-collected swab, urine, fingerstick blood | Self-collected swab or fingerstick blood |
| Time to result | 2 to 5 business days after lab receipt | 10 to 20 minutes at home |
| Sensitivity range | Mid-to-high 90s for most infections | Lower than lab NAAT, varies by kit |
| Best use | Diagnostic-grade home screening | Fast screen; confirm any positive at a lab |
| Privacy level | High (no clinic visit on file) | Highest (sample never leaves your home) |
How Accurate These Kits Are in Practice
Specific accuracy varies by infection and kit. Here is what the published data and the FDA review process say about the most common at-home tests:
Chlamydia and gonorrhea (swab-based home tests). Self-collected vaginal swabs analyzed by lab NAAT have repeatedly been shown to match clinician-collected swabs in head-to-head studies; CDC laboratory guidance identifies self-collected vaginal swabs as an acceptable specimen for chlamydia and gonorrhea NAAT. Lateral-flow rapid swab tests for chlamydia and gonorrhea sit at lower sensitivity than NAAT and are best used as a screening step. Always check the kit's product page for the specific published numbers.
HIV. The CDC's HIV testing guidance covers both rapid antibody home tests and lab-mailed fourth-generation antigen-antibody panels. Rapid antibody home tests detect HIV reliably about 23 to 90 days after exposure (the antibody window). Fourth-generation lab tests close the window faster (about 18 to 45 days) because they detect both p24 antigen and antibodies. Both technologies report very high specificity in their FDA reviews, meaning false positives are uncommon, though not impossible.
Syphilis. Home tests for syphilis are typically two-step: a screening assay (treponemal or non-treponemal antibody) followed by a confirmatory test on any positive. Lateral-flow rapid syphilis tests detect antibodies, which take 3 to 6 weeks after exposure to develop reliably; this is the window where a too-early test can miss an early infection.
Hepatitis B and C. Both are antibody-based for screening, with confirmatory antigen or RNA testing on a positive. Window periods are longer (8 to 12 weeks for hepatitis C antibody, somewhat shorter for hepatitis B), and home tests reflect the same chemistry as the in-clinic version.
Herpes (HSV-1 and HSV-2). Home herpes tests are blood antibody tests, the same type and class your provider would order. They confirm seroconversion (your body has made antibodies to the virus) but do not detect an active outbreak or specify the body site. For an active sore, a clinician-administered swab tested by PCR is the right tool, because it identifies the virus directly from the lesion.
Window-period timing applies the same way at home as at a clinic, which the next section covers.

Window Periods: Why Timing Often Matters More Than Brand
The single most common reason a real infection shows up as a negative test is testing too soon after exposure, not a faulty kit. Every infection has a window period: the time between exposure and when the test can reliably detect it. Test inside the window, and even a perfect kit will read negative.
If your exposure was recent and you test too early, a negative result is reassuring only for the time before that test. The honest practice is to retest after the longest end of the relevant window if the exposure event matters to you. This is true at a clinic and equally true at home; the kit does not change the underlying immunology.
The opposite trap also exists: antibody-based tests can stay positive for months or years after a successful treatment, even though the infection is gone. This is normal antibody chemistry, not a kit defect. If you have been treated for syphilis or HIV in the past, talk with a clinician about how to interpret a follow-up test before reading the home result on its own.
Approximate detection windows that the CDC's STI testing recommendations cite:
| Infection / test type | Approximate detection window after exposure |
|---|---|
| Chlamydia and gonorrhea (NAAT swab) | 1 to 2 weeks |
| HIV (4th-generation antigen-antibody, lab) | 18 to 45 days |
| HIV (rapid antibody, home) | 23 to 90 days |
| Syphilis (treponemal antibody) | 3 to 6 weeks |
| Hepatitis B (antibody) | 4 to 12 weeks |
| Hepatitis C (antibody) | 8 to 12 weeks |
| Herpes (HSV-2 blood antibody) | 6 to 12 weeks (rare extension to 16 weeks) |
Where Self-Collection Goes Wrong
The other realistic failure mode is sample-collection error. The kit reads what you give it; if the sample is contaminated, taken from the wrong site, or insufficient, the result is unreliable.
Common pitfalls:
- Wrong-site swab. Genital home kits are validated for vaginal or penile swabs. They are not validated for throat or rectal samples, even for the same infection. If the exposure of concern was oral or anal, a clinic-administered swab from the right site is the right tool.
- Insufficient swab time. Vaginal NAAT swabs typically need 20 to 30 seconds of contact with the vaginal wall, rotated to capture cells. A quick dab is not enough material, and the lab may report "insufficient sample" or run the test and miss a low-level infection.
- Underfilled fingerstick. Rapid blood tests have a marked fill line. Underfilling drops the test below its validated reaction volume; results in this state are unreliable. Squeeze the finger gently from the base, not the tip, and refill from a second drop if needed.
- Reading the cassette too early or too late. Lateral-flow tests have a defined read window (typically 10 to 20 minutes). A faint line that appears at 60 minutes is not a positive; it is an evaporation artifact, and most kits' instructions say so explicitly.
- Storing the kit incorrectly. Cassettes and reagents have temperature ranges. A kit that sat in a hot car for a week before you used it may not perform to spec.
Most of these are fixable by reading the instruction sheet carefully and following it the first time, not the third. If you have never used a home kit before, watch the brand's instructional video; most legitimate manufacturers publish one, and a single viewing typically eliminates the most common collection mistakes.
Home tests are not for emergencies. If you have visible genital sores, severe pelvic pain, fever after recent exposure, or a known partner with an active infection, see a clinician the same week. Home kits screen well; they do not replace urgent care, and they do not perform throat-swab or rectal-swab testing. Those samples need a clinic visit. For exposures where post-exposure prophylaxis (PEP) might be warranted, the 72-hour clock starts at exposure, not at result, so call a clinic first and test on the standard schedule afterward.
How to Pick the Right Kit for Your Situation
The right kit depends on what you actually need to know. The four most useful questions to answer before clicking buy:
1. What was the exposure? A single new partner with no symptoms in either of you is a different situation from multiple partners over the past few months. The first calls for a focused 2-in-1 or 3-in-1 panel; the second calls for a broader 7-in-1 or 8-in-1 combo.
2. How long ago was the exposure? If it was less than 2 weeks ago and you are worried about HIV or syphilis, even a perfect test today can miss the infection because of window-period timing. Either wait, or test now to establish a baseline and retest after the window closes.
3. Do you need a fast read or a definitive result? For peace of mind tonight, a lateral-flow rapid kit gives a 15-minute answer with the understanding that any positive needs lab confirmation. For a definitive answer you can act on without a second test, a mail-in lab kit is the cleaner path.
4. Are you screening or following up? Routine screening every few months for sexually active people is well-served by a multi-infection panel. A single targeted test (chlamydia only, gonorrhea only, syphilis only) makes sense after a specific known exposure where the relevant infection is already narrowed down.
If your situation is "I had a new partner recently and I want to rule out the common infections," a 3-in-1 chlamydia, gonorrhea, and syphilis panel is a sensible default. If your concern is broader (multiple partners, longer time horizon, want a baseline), a 7-in-1 covers more ground in a single shipment.
Disclosure: this article is published by stdrapidtestkits.com, which sells at-home STI testing kits. The product links below go to our own catalog. We recommend kits based on fit-for-purpose for the reader's concern, not commercial benefit.

What to Do When Your Results Come Back
The most important step in any STI test is what happens after you get the result. The home kit is a tool; it does not act on its own.
If the result is negative and your exposure was outside the window period, you can take that result at face value. If the exposure was recent and inside the window, the negative is reassuring only for what could have been detected at the time of the test; retest after the longest end of the relevant window for full coverage.
If the result is positive, two things matter. First, do not start treatment based on a home rapid test alone. Lateral-flow rapid kits have lower analytical sensitivity than lab NAAT, and even mail-in lab kits use confirmatory testing on positive screens for a reason: false positives are rare but not zero, and the wrong antibiotic for the wrong infection is a real harm. Confirm at a clinic or with a follow-up lab test before starting any treatment.
Second, plan for partner notification. WHO guidance on STI control consistently centers partner treatment as the way to break transmission cycles. Most U.S. states and many national health systems run free anonymous partner-notification services, where a public-health nurse or clinician contacts past partners on your behalf without naming you. Most clinicians can also help arrange that referral if you would prefer a single point of contact.
If you have never been tested before and you are not sure how to talk to a clinician about a positive result, the standard scripted version is short: "I tested at home and the result was positive for X. I would like a confirmatory lab test and treatment." Most clinics handle that conversation several times a week.
When to Skip the Home Kit and See a Clinic
Home testing is the right tool for screening, baseline checks, and routine retesting. There are situations where a clinic visit is genuinely the right next step, and pretending otherwise wastes time:
- Throat or rectal exposure of concern. Home kits are validated for genital and blood samples only. Pharyngeal and rectal NAATs need a clinician-collected swab from the actual site of exposure.
- Visible lesions, sores, or active outbreak. An active herpes lesion or a syphilitic chancre is best tested by direct PCR or dark-field microscopy from the lesion itself, not a blood antibody test.
- Pregnancy or planning pregnancy. Routine prenatal STI screening at a clinical lab is the standard, and most insurance covers it without a home kit being needed in the loop.
- Recent serious exposure where post-exposure prophylaxis (PEP) is on the table. HIV PEP works best when started within 72 hours of exposure. Do not wait on a home test result; go to a clinic or urgent-care center and discuss PEP first, then test on the standard schedule afterward.
- Symptoms in the urinary tract, pelvis, or testicles. Pain, discharge, or burning needs a same-week clinical evaluation that a home kit cannot substitute for.
A clinician visit for those situations also opens the conversation about PEP timing and test-of-cure follow-up, which a home kit cannot address.
Use this short check before relying on a home kit alone:
- Throat or rectal exposure of concern, where a site-specific clinician-collected swab is required.
- Visible genital lesions, sores, or an active outbreak that needs direct PCR or dark-field microscopy from the lesion.
- Pregnancy or planning pregnancy, where prenatal screening through a clinical lab is the standard of care.
- Recent serious exposure where HIV PEP may be warranted; the 72-hour PEP window starts at exposure.
- Active urinary, pelvic, or testicular symptoms (pain, discharge, burning) that need a same-week evaluation.
If any of these apply, book the clinic visit first and use a home kit only as adjunctive screening afterward.
The Bottom Line on Home STD Kit Reliability
At-home STD kits are reliable when you treat them as the tools they are. Lab-mailed kits use the same chemistry as a clinic and are diagnostic-grade when the sample is collected correctly. Rapid lateral-flow kits trade some sensitivity for speed and privacy, and they earn their place as a screening step that flags most cases quickly. Both fail in the same predictable ways: tested too early, sample collected wrong, or used for the wrong site of exposure. Pick the right kit for what you need to know, test inside the right window, follow the instructions on the first try, and confirm any positive at a lab before starting treatment.

Frequently asked questions
- Are at-home STD tests as accurate as clinic tests?
- It depends on the kit type. Lab-mailed home kits process your sample through a CLIA-certified laboratory using the same molecular and antigen-antibody methods a hospital lab runs, and they reach clinic-grade sensitivity for most infections when the sample is collected correctly. Rapid lateral-flow cassettes you read at home trade some of that sensitivity for speed and privacy; they are best treated as a screening step, with any positive confirmed at a clinic lab before treatment.
- Which STDs can I actually test for at home?
- The most common at-home options cover chlamydia and gonorrhea (self-swab), HIV (fingerstick blood), syphilis (fingerstick blood), hepatitis B and C (fingerstick blood), and HSV-1 and HSV-2 (fingerstick blood antibody). HPV and trichomoniasis at-home swabs are validated for female anatomy only; throat and rectal samples need a clinic visit.
- Do I need a prescription to buy a home STD kit?
- No. FDA-cleared home STD kits sold direct-to-consumer in the U.S. do not require a prescription. Some kits include an optional telehealth consultation if you would like clinical follow-up after a result.
- How long after exposure should I wait before testing?
- Window periods vary by infection. Roughly: 1 to 2 weeks for chlamydia and gonorrhea NAAT, 18 to 45 days for fourth-generation HIV testing (longer for rapid antibody), 3 to 6 weeks for syphilis antibody, and 8 to 12 weeks for hepatitis C. Test inside the window for a baseline, then retest after the window closes for a definitive result.
- Can a home kit give a false positive?
- Yes, although it is uncommon for FDA-cleared kits. Reported specificity is typically above 99%, meaning fewer than 1 in 100 uninfected people get a false positive. The recommended practice is to confirm any positive home result with a clinical lab test before starting treatment.
- Will the package say STD test on it?
- No. Reputable home STI kit retailers ship in plain unmarked boxes with a generic shipping label, both for privacy and because postal regulations do not require diagnostic labeling on outer packaging.
- Are home STD kits covered by insurance?
- Coverage varies. Many U.S. plans accept HSA and FSA cards for home testing kits, and some lab-processed mail-in services bill insurance directly. Check your specific kit and plan; rapid at-home kits are typically out-of-pocket.
- How often should I retest if I am sexually active?
- CDC general guidance for sexually active adults under 25, or those with new or multiple partners, is annual screening at minimum, with retesting every 3 to 6 months for higher-risk situations. Home kits make this cadence considerably easier to maintain than scheduled clinic visits.
- U.S. Centers for Disease Control and Prevention. STI screening guidance, laboratory testing recommendations, and gold-standard reference methods for chlamydia, gonorrhea, syphilis, and trichomoniasis.
- U.S. Centers for Disease Control and Prevention. HIV testing overview including fourth-generation antigen-antibody and rapid antibody home test windows.
- U.S. Food and Drug Administration. Medical devices section covering home-use diagnostic test review process, clearance requirements, and clinical performance reporting standards.
- World Health Organization. Sexually transmitted infections fact sheet covering global incidence, screening, and partner notification.
- U.S. National Library of Medicine, MedlinePlus. Sexually transmitted infections overview and patient-information reference for home and clinical testing.
- UK National Health Service. Sexually transmitted infections information, including testing and home-testing guidance.
